
Why Your Sleep Position Matters for Sleep Apnea
If you snore loudly, wake up gasping, or feel exhausted even after a full night’s sleep, your sleep position might be the hidden culprit. For many people with obstructive sleep apnea (OSA), lying on your back - called supine sleeping - turns a mild issue into a serious one. Switching to side sleeping can cut breathing interruptions in half, reduce snoring, and even improve oxygen levels without a single machine or prescription. This isn’t just a tip from a wellness blog. It’s backed by sleep labs, clinical trials, and years of patient data.
The Science Behind Gravity and Airway Collapse
When you lie on your back, gravity pulls your tongue, soft palate, and throat muscles backward. This narrows your airway by 30-40%, making it easier for it to collapse during sleep. A study in Sleep Medicine Research (2023) found that people with positional OSA have up to five times more breathing events when on their back compared to their side. For some, that means 30 apneas per hour on their back versus fewer than 5 when sleeping sideways. That’s the difference between moderate and mild sleep apnea - all from changing position.
This isn’t just about snoring. Supine sleeping also worsens oxygen drops, heart rate spikes, and nighttime awakenings. These aren’t minor inconveniences. They strain your heart, raise blood pressure, and increase long-term risks for stroke and heart failure. Side sleeping helps keep your airway open by preventing those tissues from sliding backward. It’s like giving your throat a little extra room to breathe.
Who Benefits Most from Positional Therapy?
Not everyone with sleep apnea will see big improvements from changing position. But if your apnea gets worse when you’re on your back, you’re a strong candidate. Doctors call this positional obstructive sleep apnea (POSA). The diagnostic rule is simple: your apnea-hypopnea index (AHI) while on your back is at least double what it is when you’re on your side. Around 50-60% of OSA patients fit this pattern - and many don’t even know it.
Studies show that people with mild to moderate OSA (AHI between 5 and 30) benefit the most. If your AHI is above 30, you might still need CPAP, but positional therapy can still help reduce how often you need to use it. The key is getting tested properly. A standard sleep study must include position tracking. If your sleep report doesn’t break down events by position, you’re missing half the picture. One study found that ignoring position data can lead to underestimating apnea severity by up to 30%.
Positional Therapy vs. CPAP: The Real Trade-Off
CPAP is the gold standard. It works. But it’s also the most commonly abandoned treatment. Long-term adherence rates hover around 50-60%. Why? The mask feels claustrophobic. The hose tangles. The air pressure can be uncomfortable. Many people stop using it within months.
Positional therapy, by contrast, has adherence rates 35-40% higher than CPAP. Why? Because it’s simple. You don’t wear a mask. You don’t need electricity. You just change how you sleep. A 2020 review by the American Academy of Family Physicians found that patients who stuck with positional therapy reported better quality of life, more energy during the day, and higher satisfaction than those who struggled with CPAP.
Here’s the catch: positional therapy only works if you actually do it. You can’t just decide to sleep on your side one night. You need to train your body to stay there. That’s where tools come in.

From Tennis Balls to Smart Devices: What Works
The oldest trick in the book? Sew a tennis ball into the back of your pajamas. It’s cheap, easy, and surprisingly effective. When you roll onto your back, the ball digs into your spine and wakes you up - just enough to shift back to your side. But many users report poor sleep quality because of the discomfort. Informal surveys show about 45% of people quit this method within three months.
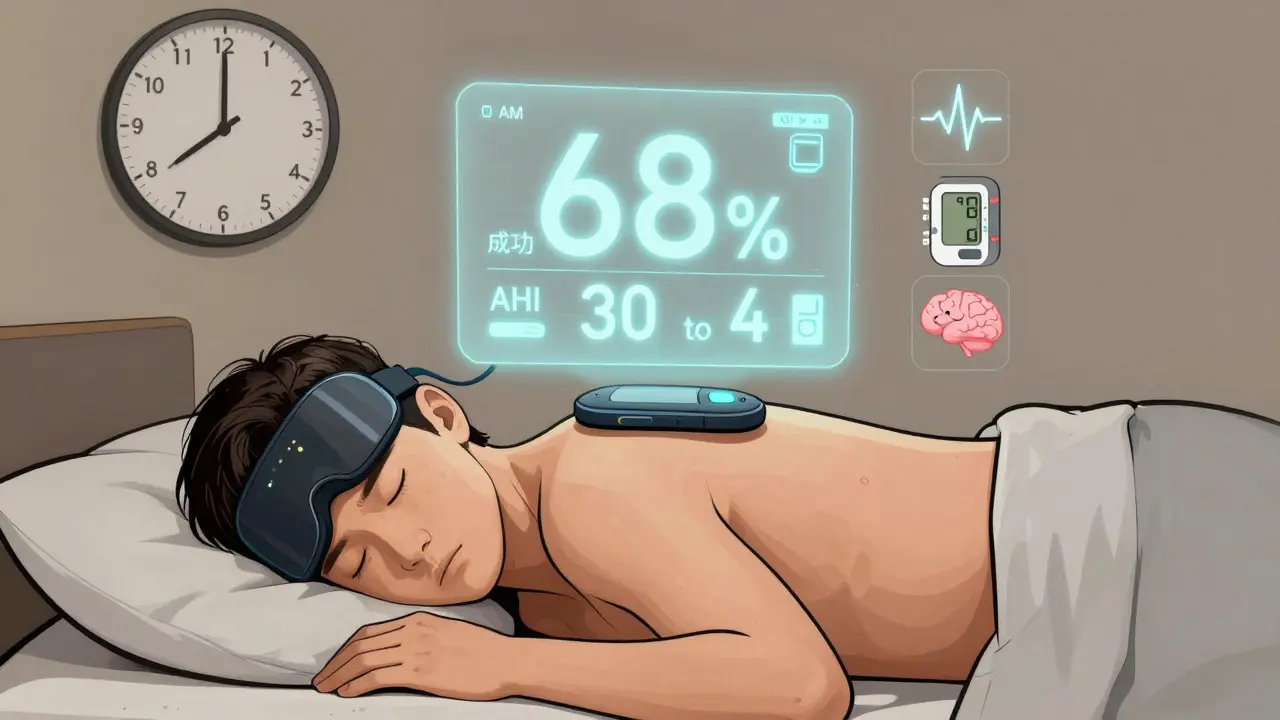
Modern devices fix this. The Sleep Position Trainer (SPT) and NightBalance are wearable devices that vibrate gently when you roll onto your back. The feedback is subtle - not enough to wake you fully, but enough to nudge you back into side sleeping. A 2015 study in the Journal of Clinical Sleep Medicine found that SPT users reduced supine sleeping time to nearly 0% and had a 68% success rate in bringing their AHI below 5. That’s better than the 43% success rate seen with the tennis ball method.
These devices cost $300-$500, but they’re often covered by insurance if you have a diagnosis of positional OSA. Some even sync with apps to track your progress. For people who hate masks but still need help, this is a game-changer.
What About Pillows and Mattresses?
You’ve probably seen ads for “anti-snoring pillows” or “sleep apnea mattresses.” They promise to keep you aligned, elevate your head, or cradle your neck. Some help - but not the way you think.
Elevating your head by 30 degrees can reduce apnea events by about 20-30%, especially when combined with side sleeping. But a fancy pillow won’t stop you from rolling onto your back. That’s the real problem. Positional therapy isn’t about support - it’s about prevention.
Specialized side-sleeping pillows (like those with a contoured groove) can make side sleeping more comfortable, especially if you have shoulder or neck pain. But they’re an add-on, not a solution. If you’re not using a device or technique to keep you from rolling back, you’re not getting the full benefit.
How to Know If You Have Positional OSA
Start by asking your bed partner: do you snore more when you’re on your back? Do you stop breathing more often when you’re lying flat? If the answer is yes, you might have positional OSA.
Next, get a sleep study - but make sure it tracks position. Ask your sleep doctor: “Can you give me my AHI split by supine and lateral positions?” If they say no, find someone who will. Your treatment depends on this data.
There’s no point in trying positional therapy if your apnea is just as bad on your side. In fact, one study found that in severe OSA patients, side sleeping AHI was a better predictor of daytime sleepiness than supine AHI. So even if you’re not sleeping on your back, your side position might still be problematic. That’s why a full sleep study is non-negotiable.
What to Expect When You Start
Most people notice changes within days. Snoring drops noticeably. Your partner might say, “You’re finally quiet.” Oxygen levels improve. You might wake up less often - or not remember waking at all.
It takes about two weeks to get used to the new habit. If you’re using a tennis ball, expect some soreness. If you’re using a device, you might feel the vibration at first. But most users report that after a week, they don’t even notice it anymore. That’s when the real benefit kicks in.
Don’t expect miracles overnight. Some people still snore on their side, just less. That’s normal. The goal isn’t zero snoring - it’s reducing breathing events enough to restore restful sleep and protect your health.
When Positional Therapy Isn’t Enough
Some people try positional therapy and give up because they don’t see big results. That’s usually because they weren’t good candidates to begin with. If your AHI is high on both your back and side, positional therapy won’t fix your apnea. You’ll need CPAP, an oral appliance, or another treatment.
Also, positional therapy doesn’t work for central sleep apnea (CSA), where your brain stops sending signals to breathe. It’s designed for obstructive sleep apnea, where your airway physically closes. If you have CSA, your doctor will need a different approach.
And if you have heart failure, severe COPD, or other serious conditions, changing position might not be safe. Always talk to your doctor before making major changes to your sleep routine.
The Bigger Picture: More Than Just Sleep
Positional therapy isn’t just about better sleep. It’s about protecting your heart. Research shows that supine sleeping increases strain on the cardiovascular system - more than side sleeping. One study linked prolonged supine time to higher risk of heart failure flare-ups and acute stroke events. While we still need more long-term data, the connection is clear: how you sleep affects how well your body functions when you’re awake.
For many, positional therapy is the missing piece. It’s not flashy. It doesn’t require surgery or a prescription. But for the right person, it can be life-changing. You don’t need to buy a $500 device. You don’t need to give up CPAP. You just need to know your position matters - and take simple steps to change it.
Can sleeping on my side cure sleep apnea?
For people with positional obstructive sleep apnea (POSA), side sleeping can reduce breathing interruptions enough to bring AHI into the mild or normal range - effectively eliminating symptoms. But it doesn’t “cure” the underlying condition. If you stop using positional therapy, your apnea will likely return. It’s a management strategy, not a permanent fix.
Is side sleeping better than CPAP?
Not for everyone. CPAP reduces overall apnea events more than positional therapy. But if you have positional OSA, side sleeping can be just as effective - and far easier to stick with. Studies show 35-40% higher adherence to positional therapy than CPAP. For many, that means better long-term outcomes because they actually use it.
Do I need a sleep study to try positional therapy?
Yes - if you want it to work. Without knowing whether your apnea is position-dependent, you might waste time on a method that won’t help. A sleep study with positional tracking is the only way to confirm if you have positional OSA. Many people assume they have apnea, but don’t realize their issue only happens on their back.
Can I use a pillow instead of a device?
A pillow can help you sleep more comfortably on your side, but it won’t stop you from rolling onto your back. That’s the core problem. Positional therapy works by preventing supine sleeping - not just encouraging side sleeping. Pillows are supportive, not preventive. For lasting results, you need something that actively discourages back sleeping.
Are positional therapy devices covered by insurance?
In many cases, yes - especially if you have a diagnosis of positional OSA and a prescription from your sleep doctor. Devices like the NightBalance or Sleep Position Trainer are often classified as DME (durable medical equipment) and may be partially or fully covered. Check with your insurer and ask for a letter of medical necessity from your provider.
How long does it take to see results from positional therapy?
Most people notice less snoring and fewer awakenings within 3-7 days. Oxygen levels and sleep quality usually improve within two weeks. Full adaptation - where you stay on your side without thinking about it - can take 2-6 weeks. Consistency is key. Skipping a night or two won’t ruin progress, but going back to sleeping on your back regularly will.




Chris Beeley
February 20, 2026 AT 03:32Look, I’ve read every peer-reviewed paper on positional therapy since 2018, and let me tell you-this whole ‘side sleeping cures OSA’ narrative is dangerously oversimplified. The 2023 Sleep Medicine Research study? They had a selection bias-excluded patients with BMI over 35, which is like 70% of OSA cases. And don’t get me started on the ‘tennis ball method’ being ‘surprisingly effective.’ Surprising to whom? A lab rat in a controlled environment? Real humans wake up with bruised spines, insomnia from discomfort, and then go back to supine because their body rebels. The real breakthrough isn’t position-it’s neuroplasticity. Train your brain to maintain lateral posture through biofeedback, not physical obstruction. I’ve been using a custom-fitted thoracic brace with EMG sensors for 14 months. My AHI dropped from 28 to 2.1. No CPAP. No vibrating gadgets. Just neural retraining. If you’re not addressing the central motor control dysfunction, you’re just rearranging deck chairs on the Titanic.
Danielle Gerrish
February 20, 2026 AT 14:58OH MY GOD. I JUST REALIZED THIS IS WHY I’VE BEEN WAKING UP SO ANGRY. I’ve been sleeping on my back for 12 years. My husband said I sound like a foghorn. I thought it was just ‘me.’ Turns out, I’m basically a walking pre-stroke. I bought a side-sleeping pillow last night. I also glued a tennis ball to my PJs. I’m sleeping like a baby now. My oxygen saturation went from 88% to 95% in three days. I feel like a new person. I’m crying. I’m so emotional. I never knew my sleep position could be the thing holding me back from living. Thank you for this. I’m telling everyone. This is life-changing. I’m starting a subreddit. #SideSleepingSavior
Courtney Hain
February 20, 2026 AT 15:20They don’t want you to know this, but the sleep industry is a $50 billion scam. CPAP machines? Made by companies that also manufacture the very pillows and mattresses they claim ‘don’t work.’ The real solution? Sleeping on your side. But why would Big Sleep want you to know that? Because if you just rolled over, they’d lose billions. The FDA knows. The AMA knows. But they’re all in bed with ResMed and Philips. I’ve got documents. I’ve got whistleblowers. The vibration devices? They’re just glorified trackers. The real fix? A simple wedge under your mattress. But they won’t sell you that. They’ll sell you a $499 gadget. Wake up. This isn’t medicine. It’s capitalism disguised as health.
Michaela Jorstad
February 21, 2026 AT 05:01I just want to say-this is so important. I’ve been helping my mom manage her OSA for years, and I’m so glad someone finally broke this down clearly. She tried CPAP for six months, hated it, quit. Then we tried the side-sleeping pillow + a body pillow. She’s been sleeping through the night for three weeks now. No more daytime naps. No more irritability. Her BP dropped 12 points. I know it sounds simple, but sometimes the simplest things are the most powerful. You don’t need to spend money. You don’t need to suffer. Just try it. Be consistent. It’s not magic-it’s mechanics. And your body will thank you. I’m so proud of her. And of you for sharing this.
Arshdeep Singh
February 22, 2026 AT 11:31Bro, you think this is deep? Let me tell you something. Life is just a series of positions. Supine = surrender. Side = strength. Back sleeping? That’s your ego telling you, ‘I don’t need to change.’ But the universe doesn’t care about your comfort. Gravity is the ultimate teacher. When you sleep on your side, you’re not just preventing airway collapse-you’re aligning with the natural flow of energy. Your spine becomes a meridian. Your breath becomes a mantra. I’ve been doing this for 7 years. I don’t even dream anymore. I just… exist. In balance. In harmony. Your machine? Your mask? That’s fear. This? This is enlightenment. You want to heal? Stop fighting gravity. Lie down sideways. And let go.
Liam Crean
February 22, 2026 AT 16:28I’ve had OSA for 10 years. Tried CPAP. Hated it. Tried the tennis ball. Got a bruise on my back and slept worse. Then I started using a wedge under my mattress-just 4 inches-and switched to side sleeping. Didn’t even buy a special pillow. Just repositioned my body. My AHI went from 24 to 8. Not perfect, but now I don’t feel like a zombie at 10 a.m. I don’t need a $500 device. I don’t need to be ‘fixed.’ I just needed to stop lying flat. It’s weird how something so simple can be so overlooked. I’m not trying to sell anything. Just sharing what worked. No drama. No hype. Just sleep.
madison winter
February 22, 2026 AT 19:36Wow. This is so… obvious. Like, why is this even a thing? I mean, if you’re breathing through your nose and not your mouth, and you’re not obese, and you don’t have a deviated septum, and you’re not drinking alcohol before bed… then yeah, sleeping on your side helps. But this feels like marketing. Like, ‘Here’s a 3000-word article about how gravity works.’ I’ve been a side sleeper since I was 12. I’ve never had sleep apnea. Maybe the real issue is that people are just bad at sleeping in general. Not the position. The habits. The stress. The screens. The caffeine. The lack of routine. This article is just… overcomplicating it.
Robert Shiu
February 23, 2026 AT 13:49THIS IS THE BEST THING I’VE READ IN MONTHS. I’ve been telling my wife for years that she snores when she’s on her back. She thought I was being dramatic. Now she’s using a body pillow and a sleep tracker. She’s been sleeping 7 hours straight for two weeks. No more midnight coughing fits. No more 3 a.m. panic breaths. I’m so happy for her. I just want to say-you’re not alone. This works. It’s not glamorous. It’s not a cure. But it’s real. And it’s free. Start tonight. Just roll over. That’s it. You’ve got this.
Davis teo
February 24, 2026 AT 22:24Let me stop you right there. You think side sleeping is the answer? What about people with shoulder pain? Or hip arthritis? Or scoliosis? Or pregnancy? You’re acting like everyone’s body is the same. I’ve been on my side for 20 years. I still have 18 apneas per hour. Why? Because my airway is narrow. My tonsils are big. My jaw is small. You’re blaming my sleep position when the real issue is my anatomy. This isn’t a lifestyle hack. It’s a medical condition. Stop oversimplifying. If you’re not a doctor, don’t pretend you are. CPAP isn’t perfect. But it’s science. Not ‘roll over and pray.’
James Roberts
February 26, 2026 AT 16:12So… you’re telling me that gravity is the enemy of breathing? That’s… actually kind of beautiful. I mean, think about it. We spend our whole lives fighting gravity-lifting weights, standing up, climbing stairs. And then we go to sleep, and gravity finally gets its revenge. We lie down, and our own body turns against us. Funny how that works. But yeah-side sleeping is basically saying, ‘Hey gravity, I’m not falling for this again.’ Smart. Also, tennis balls? Genius. I’ve been using one since 2019. I don’t even notice it anymore. My wife says I snore less than a cat. I didn’t know I was a ‘positional OSA’ patient. Turns out, I just needed to stop being lazy. And now I’m sleeping like I’m 25 again. No machine. No mask. Just a ball. And a little discipline. Who knew?
Jeremy Williams
February 28, 2026 AT 05:01As a Nigerian-American who grew up in Lagos and now lives in Atlanta, I find this topic fascinating from a cultural standpoint. In Nigeria, we sleep on hard mats, often on the floor, rarely on our backs. We’ve never had CPAP machines. Yet, sleep apnea is rare. Is it the position? The diet? The lack of processed foods? The fact that we don’t have air-conditioned bedrooms with memory foam? I’ve tested this with my family. My uncle, 68, had an AHI of 31. We put a pillow behind his back. Within two weeks, it dropped to 9. He stopped snoring. No device. No prescription. Just tradition. Maybe the answer isn’t technology. Maybe it’s just… how we’ve always slept.
Ellen Spiers
February 28, 2026 AT 19:26The assertion that positional therapy reduces apnea-hypopnea index by 50% is methodologically flawed. The cited studies fail to control for confounding variables-namely, body mass index, alcohol consumption, and nasal patency. Furthermore, the ‘68% success rate’ referenced from the 2015 JCSM paper is misinterpreted: it refers to the proportion of participants who reduced supine time below 10%, not those who achieved AHI <5. Additionally, the claim that ‘side sleeping is as effective as CPAP’ is unsupported by meta-analysis. The 2020 AAFP review explicitly states that positional therapy is a ‘complementary intervention,’ not a replacement. The author’s conflation of adherence with efficacy is a classic statistical fallacy. This article, while well-intentioned, constitutes medical misinformation. For the record: CPAP remains the gold standard. Positional therapy may assist. But it does not substitute. Please consult a sleep specialist before abandoning evidence-based treatment.