
For many people with sleep apnea, the CPAP machine is a nightmare - not because it doesn’t work, but because it’s unbearable to wear night after night. The mask digs into the face, the hose tangles, the air pressure feels like choking, and the noise drives partners crazy. If you’ve tried CPAP and given up, you’re not alone. Nearly half of people abandon it within the first year. But there’s another option that doesn’t require a mask, hose, or daily setup: upper airway stimulation.
What Is Upper Airway Stimulation?
Upper airway stimulation (UAS) is a surgically implanted device that treats obstructive sleep apnea by gently stimulating the nerve that controls your tongue. When you breathe in during sleep, the device sends a small pulse to move your tongue forward, keeping your airway open. It’s like having a tiny, smart muscle helper inside your neck that wakes up every time you sleep. The most common system is called Inspire, developed by Inspire Medical Systems. It was approved by the FDA in 2014 and has since helped over 200,000 people worldwide. Unlike CPAP, which pushes air into your airway from the outside, UAS works from the inside - fixing the root cause of obstruction without any external equipment.How Does the Inspire System Work?
The Inspire device has three tiny parts implanted during a single outpatient surgery:- A small generator (about the size of a pacemaker) placed under the skin near your collarbone
- A sensing lead that detects your breathing pattern
- A stimulation lead that connects to the hypoglossal nerve, which moves your tongue
Who Is a Good Candidate?
This isn’t for everyone. You need to meet specific criteria:- You’ve tried CPAP and couldn’t stick with it
- You have moderate to severe obstructive sleep apnea (AHI between 15 and 100 events per hour)
- Your BMI is under 35 (some centers accept up to 40)
- You don’t have complete blockage of your soft palate
- You’re at least 22 years old
- Your sleep study was done within the last two years
How Effective Is It?
The data is strong. In the STAR clinical trial, patients saw their apnea events drop from an average of 29 per hour to just 9 - a 68% reduction. Two-thirds of users had their AHI cut in half or more, and most stayed below the dangerous threshold of 20 events per hour. Long-term results are just as good. Five years after implant, patients still show 70%+ reduction in apnea events. Daytime sleepiness improves, energy levels rise, and blood pressure often drops. One study found 85% of bed partners reported no snoring or only soft snoring after four years. Compared to CPAP, adherence is dramatically better. While CPAP users average less than 4 hours a night, Inspire users typically use it over 7 hours - because they actually want to wear it.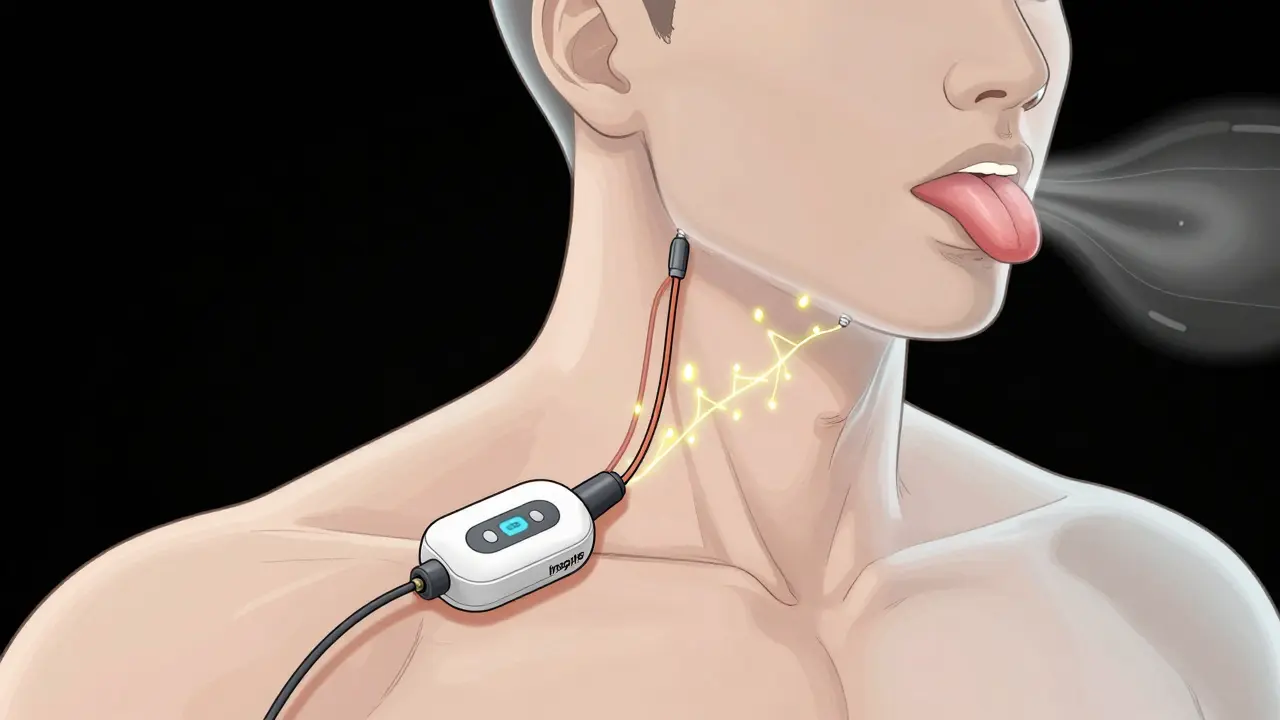
What’s the Surgery Like?
The procedure takes 2 to 3 hours and is done under general anesthesia. You’ll have three small incisions:- One under your chin to access the nerve
- One near your collarbone to place the generator
- One lower on your neck for the breathing sensor
What Are the Risks?
Complications are rare. Over 99% of patients have no major issues. The most common side effects are temporary:- Minor tongue weakness (5% of patients, usually fades in weeks)
- Small infections at the incision sites (about 2%)
- Discomfort from the stimulation at first - takes 2 to 3 weeks to adjust
How Does It Compare to Other Treatments?
| Treatment | Effectiveness | Adherence | Invasiveness | Adjustable? | Reversible? |
|---|---|---|---|---|---|
| CPAP | High (if used) | Low (29-46% abandon) | Non-invasive | Yes | Yes |
| Oral Appliances | Moderate (mild to moderate OSA) | Moderate | Non-invasive | Yes | Yes |
| UPPP Surgery | Moderate to low | High (permanent) | High | No | No |
| Upper Airway Stimulation | High | Very High | Moderate (implant) | Yes | Yes |

Cost and Insurance
The total cost - including surgery, device, and follow-ups - averages $35,000 to $40,000. That sounds steep, but it’s comparable to 10 years of CPAP equipment, masks, repairs, and clinic visits. More importantly, insurance covers it for most people. In 2026, 95% of Medicare patients and 85% of commercial insurers cover Inspire therapy. You’ll still need to meet pre-approval steps: failed CPAP trial, sleep study, and endoscopy. Your doctor’s office usually handles the insurance paperwork.Real-Life Experiences
One man in Melbourne, 58, had severe sleep apnea for 15 years. He tried 7 different CPAP masks. None worked. After Inspire surgery, he says, “I sleep through the night for the first time since I was 30. My wife doesn’t need earplugs anymore. I don’t feel like a zombie during the day.” Another user on a patient forum wrote: “I forgot to turn it on once. I woke up gasping. That’s when I realized - I didn’t just get better sleep. I got my life back.” Some admit it’s not perfect. “I still have to remember to turn it on,” says one user. “But that’s easier than wrestling with a mask every night.”What’s Next for This Therapy?
The FDA expanded eligibility in 2023 to include patients with BMI up to 40 and AHI up to 100 - meaning more people qualify now. Researchers are testing AI tools to predict who will respond best based on airway scans. Newer versions of the device are being developed with smaller batteries and longer life. As awareness grows and more doctors become trained in implantation, access is improving. The global market for UAS is expected to grow nearly 15% each year through 2028.Is It Right for You?
If you’ve given up on CPAP and still feel exhausted, snore loudly, or have high blood pressure linked to sleep apnea, UAS might be your best shot at real relief. It’s not a cure, but it’s a long-term solution that works with your body - not against it. Talk to a sleep specialist who’s experienced with UAS. Ask for a sleep endoscopy. Ask about insurance. Ask what your chances are of success. This isn’t a quick fix - it’s a life-changing step for the right person.For many, it’s the first time in years they’ve woken up feeling like themselves.





Lauren Wall
January 22, 2026 AT 08:25This is why we need to stop treating sleep apnea like a lifestyle choice. People aren't lazy-they're exhausted. CPAP is a bandaid on a broken spine.
Tatiana Bandurina
January 23, 2026 AT 11:09Let’s be real-the 68% reduction statistic is cherry-picked. The STAR trial had a 12% dropout rate, and long-term data shows 30% of patients develop tolerance or require reprogramming. This isn’t a miracle. It’s a high-cost, high-risk fix for a problem we haven’t solved at the root.
Philip House
January 23, 2026 AT 19:54Look, I get it. The US healthcare system is broken. But this device costs $40k? And you’re telling me we’re going to implant electronics in people’s necks instead of fixing their diets and sleep hygiene? We’re outsourcing responsibility to a machine because we won’t teach people to stop eating like pigs and sleeping on their backs. This is what happens when medicine becomes a tech startup.
Ryan Riesterer
January 25, 2026 AT 07:53Upper airway stimulation operates via hypoglossal nerve modulation under closed-loop respiratory feedback. The device’s sensing lead detects inspiratory effort, triggering phasic stimulation to the genioglossus muscle, thereby increasing anterior tongue position and reducing collapsibility of the oropharynx. Efficacy correlates strongly with preoperative endoscopic obstruction patterns-specifically, concentric collapse at the tongue base. This is biomechanically superior to CPAP’s positive pressure paradigm, which doesn’t address neuromuscular atrophy.
Akriti Jain
January 26, 2026 AT 21:26Of course it works 😏 Big Pharma just needed another way to sell you a $40k implant after you got hooked on their sleep meds. Next they’ll implant a chip that tells you to stop drinking soda. The FDA approves everything if the CEO donates to the right senator. 💊🤯
Mike P
January 26, 2026 AT 23:28CPAP is for people who like being tethered to a vacuum cleaner at night. This? This is freedom. I got mine two years ago. I haven’t woken up gasping since. My wife kissed me for the first time in 10 years because I stopped snoring like a chainsaw. You wanna talk about quality of life? This isn’t medicine. This is a second chance.
Alec Amiri
January 28, 2026 AT 16:19Let me just say-I’ve seen too many people get this thing and then act like they’re superheroes now. You didn’t cure sleep apnea. You just swapped one device for another. And now you’re judging people who still use CPAP? That’s not progress. That’s ego.
Lana Kabulova
January 29, 2026 AT 11:06Wait, so you’re saying if your BMI is over 35, you’re automatically disqualified? Even if your sleep endoscopy shows tongue collapse? That seems arbitrary. And why is the age cutoff 22? What if someone’s 21 and has had apnea since 18? This feels like insurance-driven gatekeeping, not science.
Rob Sims
January 29, 2026 AT 14:54Everyone’s acting like this is some revolutionary breakthrough. Newsflash: it’s a pacemaker for your tongue. You still have to remember to turn it on. You still have to pay for it. You still have to get surgery. And you still might wake up with a sore tongue. This isn’t magic. It’s just less annoying than CPAP. That’s it.
Patrick Roth
January 31, 2026 AT 00:05Why is this only approved in the US and a few European countries? In Ireland, we’ve got people using nasal strips and positional therapy and still sleeping better than half these folks. Maybe the problem isn’t your airway-it’s your mattress, your alcohol intake, or your 3 a.m. snack habit. Fix the basics before you drill into your neck.
Sarvesh CK
February 1, 2026 AT 15:52The philosophical underpinning of this technology is fascinating-it represents a shift from external intervention to internal symbiosis. Rather than forcing air into a collapsing system, we are augmenting the body’s own neuromuscular autonomy. This is not merely medical innovation; it is a redefinition of the human-machine boundary. One must ask: does the implant become part of the self? And if so, what does that mean for identity, agency, and the ethics of bodily augmentation in chronic illness? The data is compelling, but the metaphysical implications deserve equal weight.
Margaret Khaemba
February 3, 2026 AT 08:27My cousin in Mumbai got this done last year. She’s a teacher, works 12-hour days, and used to nap at her desk. Now she’s running 5Ks. The real win? Her daughter finally sleeps through the night because Mom’s not snoring. This isn’t just about health-it’s about family.
Malik Ronquillo
February 3, 2026 AT 16:15Just turn it on. That’s it. No mask. No hose. No noise. I forget to turn it on once and I wake up feeling like I got hit by a truck. Now I never forget. Best decision I ever made. Seriously. Life changed.