When you hear the word biosimilar, you might think it’s just another name for a generic drug. But that’s not true. Biosimilars aren’t copies in the same way generics are. They’re highly similar versions of complex biologic drugs - medicines made from living cells, like antibodies or proteins. These aren’t simple chemicals you can replicate exactly. That’s why the FDA doesn’t just approve them the same way it does for generics. The process is deeper, tougher, and more detailed.
What Makes Biosimilars Different From Generics?
Generics are exact copies of small-molecule drugs. Think of them like baking a cake from a recipe - if you use the same ingredients in the same amounts, you get the same cake. Biosimilars? They’re more like recreating a handmade sculpture from a photo. You can get incredibly close, but you can’t make an identical copy because the original is made by living cells, not chemicals. Even tiny differences in how those cells grow can change how the drug works. The FDA doesn’t call biosimilars "identical" - it calls them "highly similar." That’s not just wordplay. It’s the legal standard. For a biosimilar to be approved, it must show no clinically meaningful differences in safety, purity, or potency compared to the original biologic. That’s the bar. And it’s not easy to hit.The FDA’s Step-by-Step Evaluation Process
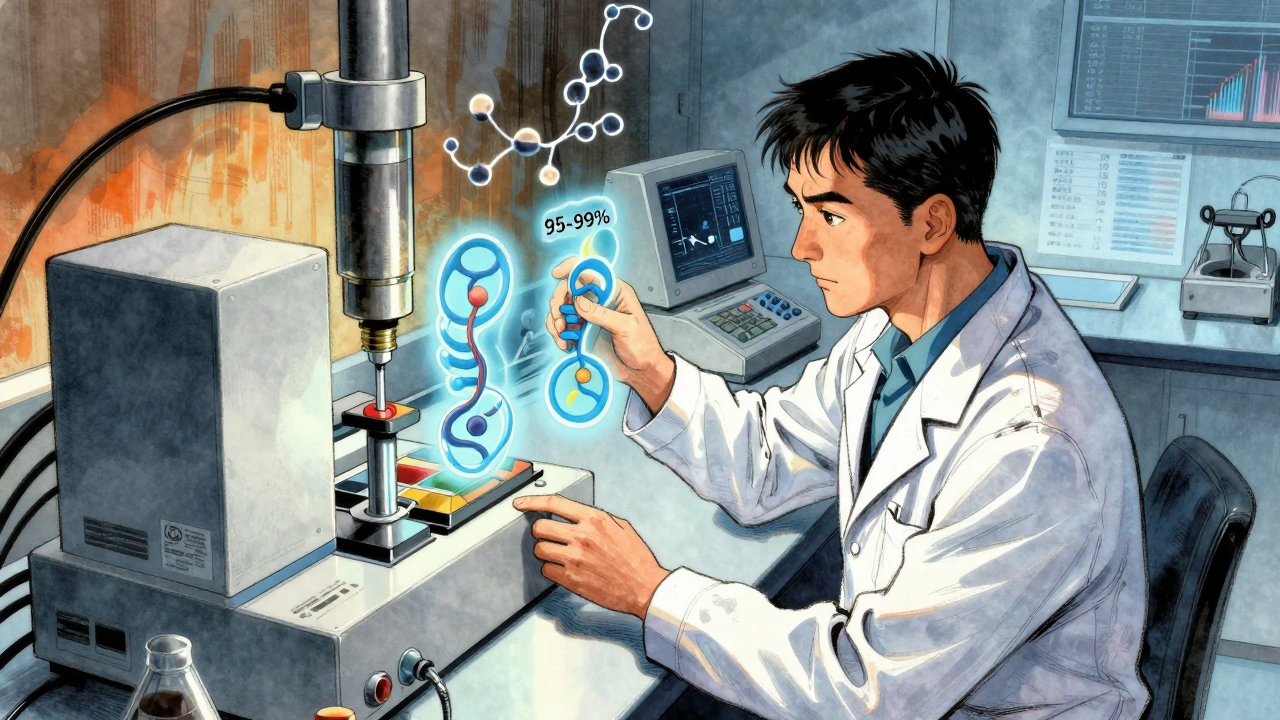
The FDA doesn’t just look at one thing. It builds a full picture using four layers of evidence, starting with the most detailed science and moving toward real-world results.- Analytical Studies: This is where most of the work happens. Labs use advanced tools - mass spectrometers, capillary electrophoresis, chromatography - to compare the biosimilar and the reference drug molecule by molecule. They look at over 200 different characteristics: shape, size, charge, sugar attachments (glycosylation), and how the protein folds. The FDA expects 95-99% similarity across these attributes. If the data doesn’t show that level of match, the application stops right there.
- Animal Studies: If the analytical data looks strong, the next step is often animal testing. This checks for toxicity and how the body responds. But here’s the twist: the FDA can skip this step if the analytical data is solid enough. That’s new. In 2024, the agency updated its guidance to allow this flexibility, which saves time and money.
- Human Studies: This is where pharmacokinetics (how the body absorbs and processes the drug) and pharmacodynamics (how the drug affects the body) are tested. Usually, this involves 50-100 healthy volunteers in a crossover study. The design is simple: half get the reference drug first, then the biosimilar. The other half gets them in reverse order. If the levels in the blood and the body’s response are nearly identical, that’s a green light.
- Immunogenicity Testing: This is critical. Biologics can trigger immune reactions - think rashes, fever, or worse. Every biosimilar must be tested over 24 to 52 weeks to make sure it doesn’t cause more immune responses than the original. The FDA tracks this through blood tests and patient reports. So far, no approved biosimilar has shown a higher risk than its reference product.
The Purple Book: The Official FDA Listing
You won’t find biosimilars listed in the same place as generics. That’s because biologics have their own directory: the Purple Book. It’s the FDA’s official list of all approved biologics - both the original drugs and their biosimilars. It’s updated daily now, thanks to a 2025 upgrade. Before, it was monthly. Now, if a biosimilar gets approved on Tuesday, it’s in the book by Thursday. The Purple Book doesn’t just list names. It shows:- Which drug is the reference product
- When the biosimilar was approved
- Whether it’s designated as "interchangeable"
- Patent information submitted by the original drugmaker
- Exclusivity periods
What Does "Interchangeable" Mean?
Not all biosimilars are created equal in the eyes of pharmacists and insurers. An "interchangeable" biosimilar meets an even higher standard. It must prove that switching between it and the reference drug - even multiple times - won’t change how safe or effective the treatment is. That’s not just about one study. It’s about data showing no increased risk from switching. In practice, this means a pharmacist can swap an interchangeable biosimilar for the original drug without asking the doctor. That’s not allowed for non-interchangeable biosimilars. Most states require a doctor’s permission for those. That’s why only 17 out of 43 have this status. Getting there takes more data, more time, and more money. But for patients and pharmacies, it’s worth it.Why Does This Take So Long and Cost So Much?
Developing a biosimilar isn’t cheap. On average, it costs $120-180 million just to run the analytical studies. That’s 30-40% of the total development cost. And it takes 10-12 months of full-time work by teams of scientists using specialized equipment. Compare that to a generic, which can be developed for under $2 million. The FDA’s standards are stricter than Europe’s. The European Medicines Agency (EMA) has approved 118 biosimilars as of 2025. The FDA has approved 43. That’s not because the U.S. is slower - it’s because the FDA asks for more data. The median approval time in the U.S. is 3.2 years. In Europe, it’s 2.1 years. Patent lawsuits also delay launch. Even after the FDA approves a biosimilar, it can sit on the shelf for years while companies fight in court. Of the 43 approved biosimilars, only 29 have actually reached the market. The average delay between approval and launch? 11.3 months.Who Benefits From Biosimilars?
Patients do. The FDA estimates biosimilars reduce costs by 15-30% compared to the original biologics. In oncology, where drugs like trastuzumab and rituximab cost $100,000 a year, that’s life-changing. In 2024, biosimilars saved the U.S. healthcare system $12.7 billion. The FDA projects that by 2030, those savings will hit $250 billion. But adoption isn’t equal. Cancer treatments? Biosimilars are taking over - 65-75% market share within 18 months. Autoimmune diseases? Much slower. Adalimumab biosimilars, approved in 2023, only reached 28% market share by mid-2025. Why? Payers and doctors are still cautious. Many patients have been on the original drug for years. Switching feels risky, even when the science says it’s not.
What’s Next for Biosimilars?
The FDA is making changes to speed things up. In 2024, it removed the requirement for forced degradation studies - tests that showed how the drug breaks down under stress. Experts said those didn’t predict real-world outcomes. In June 2025, the agency started allowing indication extrapolation based on analytical data alone for simpler proteins. That means if a biosimilar works for one condition, it can be approved for others without new trials. The next big push? Complex biosimilars - things like antibody-drug conjugates and gene therapies. Only three applications have been submitted so far. None have been approved. The FDA plans to release new guidance for these by Q3 2026. It’s also testing AI tools to help review analytical data faster. The goal is clear: get more affordable, safe biologics to patients without cutting corners. The FDA’s process may be long, but the data shows it works. Since 2015, there have been no biosimilar-specific safety signals in over 9 years of real-world use. That’s not luck. That’s science.Common Misconceptions
- "Biosimilars are just generics." No. Generics are chemically identical. Biosimilars are highly similar - but not identical - because they’re made from living cells.
- "If it’s approved, it’s interchangeable." No. Only 17 of 43 approved biosimilars have that status. The rest require a doctor’s order to switch.
- "Biosimilars are less safe." False. FDA data shows adverse event rates are statistically the same as the original biologics.
- "The FDA doesn’t test them well." The opposite is true. The analytical standards are among the most rigorous in the world.
Are biosimilars as safe as the original biologic drugs?
Yes. Since the first biosimilar was approved in 2015, the FDA has tracked over 9 years of real-world use across all 43 approved products. Adverse event rates are statistically identical to those of the reference biologics - 0.8 per 10,000 patients for biosimilars versus 0.7 for originals. No biosimilar has introduced a new safety risk.
Can a pharmacist automatically switch me to a biosimilar?
Only if the biosimilar is labeled "interchangeable" by the FDA. There are 17 interchangeable biosimilars approved as of 2025. For non-interchangeable ones, your doctor must specifically prescribe the biosimilar. State laws vary, but most require a doctor’s approval before substitution.
Why are there so few biosimilars approved in the U.S. compared to Europe?
The FDA requires more detailed analytical data than the European Medicines Agency (EMA). While the EMA has approved 118 biosimilars as of 2025, the FDA’s higher bar for similarity - especially around complex molecular structures - means longer review times and more development costs. The U.S. approval process takes about 3.2 years on average, compared to 2.1 years in Europe.
Do biosimilars work for all the same conditions as the original drug?
Not always - but often. The FDA allows "extrapolation" of indications if the biosimilar is shown to be highly similar and the mechanism of action is the same across conditions. For example, if a biosimilar works for rheumatoid arthritis, and the drug’s action is understood to be the same in Crohn’s disease, the FDA may approve it for both without new clinical trials. This is now common for simpler proteins, thanks to 2024-2025 guidance updates.
Why are some biosimilars still not on the market after FDA approval?
Patent lawsuits are the main reason. Even after the FDA approves a biosimilar, the original drugmaker can sue to delay its launch. Between 2015 and 2025, 14 out of 43 approved biosimilars were held up by litigation. The average delay between approval and market launch is 11.3 months. Some have waited over 5 years.



Levi Cooper
December 12, 2025 AT 15:06Look, I don’t care how many decimal points they measure - if a drug isn’t made in the USA, it’s not the same. The FDA’s just letting foreign labs cut corners under the guise of ‘highly similar.’ We used to make the best medicines in the world. Now? We’re accepting ‘close enough’ because some CEO wants to save a few bucks. And don’t get me started on those Indian labs - you think they’re running sterile conditions? Please.
Laura Weemering
December 14, 2025 AT 02:24...the analytical rigor, though... it’s not just about % similarity - it’s about the ontological instability of biological systems, right? The glycosylation patterns aren’t just ‘molecular noise’ - they’re epigenetic signatures of the host cell’s existential trauma... and the FDA’s reductionist metrics completely erase that phenomenological dimension... I mean, how can you quantify ‘soul’ in a chromatogram? ...
Reshma Sinha
December 16, 2025 AT 01:16This is such a clear breakdown! As someone working in biopharma R&D in India, I can tell you - the analytical standards the FDA requires are insane but necessary. We spent 14 months just on the mass spec data for our last candidate. The Purple Book update? Game-changer. Real-time transparency = faster trust. More biosimilars = more patients get treated. Let’s keep pushing this forward! 💪
nikki yamashita
December 17, 2025 AT 14:22Rob Purvis
December 18, 2025 AT 17:28Just to clarify - when the FDA says ‘no clinically meaningful differences,’ that’s not just a phrase. It means: if a patient switches from the originator to the biosimilar, their outcomes - hospitalizations, side effects, lab markers - should be statistically identical. And the data backs it. I’ve reviewed 12 of these applications. The level of detail? Mind-blowing. They’re not cutting corners. They’re just being smarter.
Stacy Foster
December 20, 2025 AT 01:29Let’s be real - this whole biosimilar system is a pharmaceutical scam. The FDA’s ‘rigorous’ process? A front. The real reason they approve these is because Big Pharma bribes regulators to let cheaper drugs in so they can jack up prices on the originals. And those ‘interchangeable’ labels? Pure marketing. They’re forcing patients into switches to save insurance money - not for their safety. I’ve seen people get sick after switching. They just don’t report it. The system is rigged.
Lawrence Armstrong
December 20, 2025 AT 20:36Just wanted to add - the 95-99% similarity isn’t arbitrary. It’s based on decades of clinical data showing that below 95%, you start seeing immune responses. Above 99%, you’re not gaining anything meaningful. Also - AI tools are now being used to flag anomalous glycosylation patterns that humans might miss. It’s not magic. It’s math + biology. 🤖🧬
Audrey Crothers
December 22, 2025 AT 06:22Y’all are overcomplicating this. Biosimilars = same result, way cheaper. Period. 💸 My cousin got her cancer drug for $30K instead of $100K. She’s alive. That’s all that matters. If the FDA says it’s safe, trust them. Stop arguing and let people get better.