When a basketball player suddenly stops short and feels a sharp click deep in the hip, or a soccer player can’t sprint without pain, it’s often not a muscle strain. More often, it’s a hip labral tear. This injury doesn’t show up on regular X-rays. It doesn’t always show on standard MRIs. But for athletes under 40, especially those in sports that demand twisting, pivoting, and deep hip flexion, it’s one of the most common - and most misunderstood - sources of chronic hip pain.
What Exactly Is the Hip Labrum?
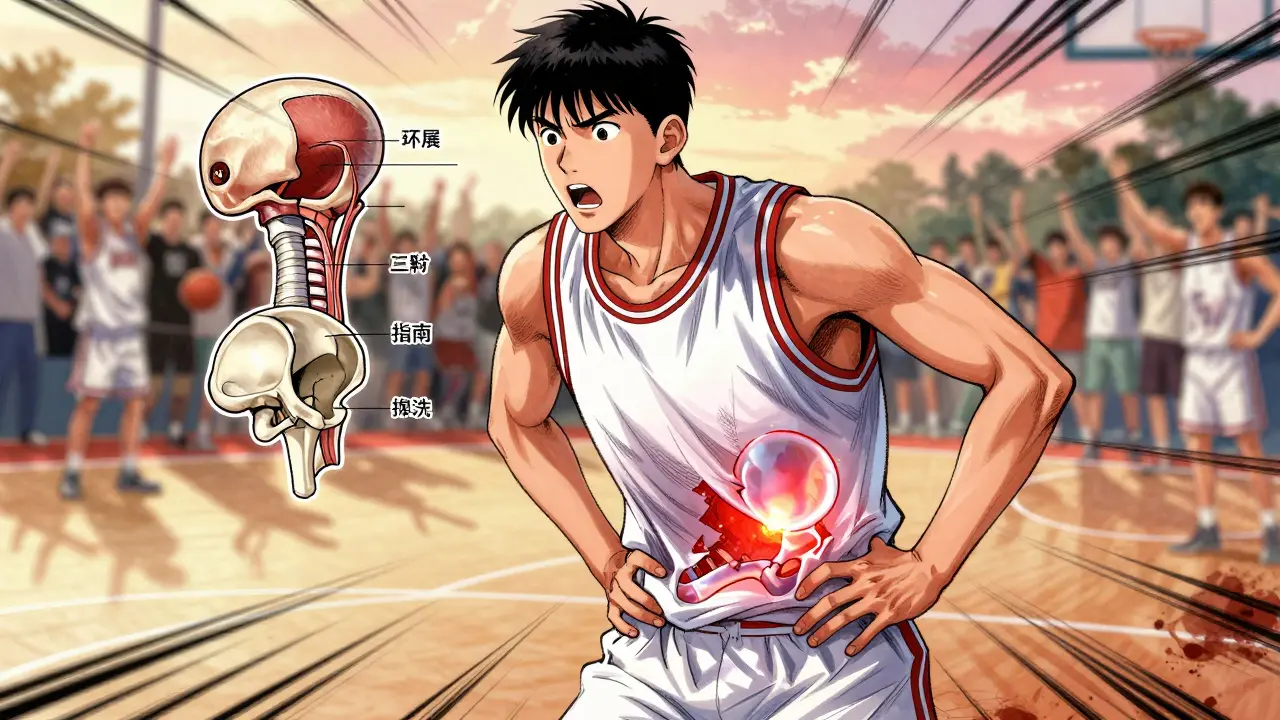
The labrum is a ring of tough, rubbery cartilage that wraps around the outside of the hip socket (acetabulum). Think of it like a seal around a jar lid - it helps hold the ball of the femur securely in place, adds stability, and cushions the joint. When this ring tears, it doesn’t just hurt; it can cause clicking, locking, or a deep ache that worsens with activity. It’s not a simple wear-and-tear injury. In athletes, it’s usually the result of repeated stress or an underlying structural issue like femoroacetabular impingement (FAI), where the bones of the hip rub abnormally against each other.Who Gets Hip Labral Tears - And Why?
You don’t have to be a pro to get one. But your risk shoots up if you play sports that involve sudden changes in direction, deep squats, or extreme hip rotation. Basketball, soccer, hockey, gymnastics, and ballet top the list. A 2022 study found these four sports account for more than 70% of diagnosed cases in athletes. Younger athletes - under 35 - are most affected. Why? Their bodies are pushing harder, faster, and more frequently than ever before. And often, they’ve had subtle hip misalignments since childhood that only become problematic under athletic stress.How Is It Diagnosed? Imaging Isn’t Always Enough
A doctor won’t just look at your hip and guess. Diagnosis starts with physical tests. The FADIR test (flexion, adduction, internal rotation) and the FABER test (flexion, abduction, external rotation) are standard. If these trigger sharp pain or a catching sensation, it’s a red flag. But imaging is where things get precise. Plain X-rays are the first step - they check for bone shape problems like FAI or hip dysplasia. But they won’t show the labrum. Standard MRI? It misses up to 30% of tears. That’s why magnetic resonance arthrography (MRA) is now the gold standard for imaging. MRA involves injecting contrast dye into the hip joint before the scan. This makes the labrum stand out clearly. Studies show MRA detects labral tears with 90-95% accuracy. Without it, you’re flying blind.Arthroscopy: The Only Way to Know for Sure
Even MRA isn’t perfect. Sometimes, the tear looks minor on the scan but is more severe in reality. That’s why hip arthroscopy remains the definitive diagnostic tool. During the procedure, a tiny camera is inserted into the joint. The surgeon sees the labrum directly. They can confirm the tear, assess its size and location, and check for other problems - like loose cartilage, synovitis, or bone spurs - that often come with it. In fact, arthroscopy has a 98% accuracy rate. If you’re considering surgery, this is the moment you get the full picture.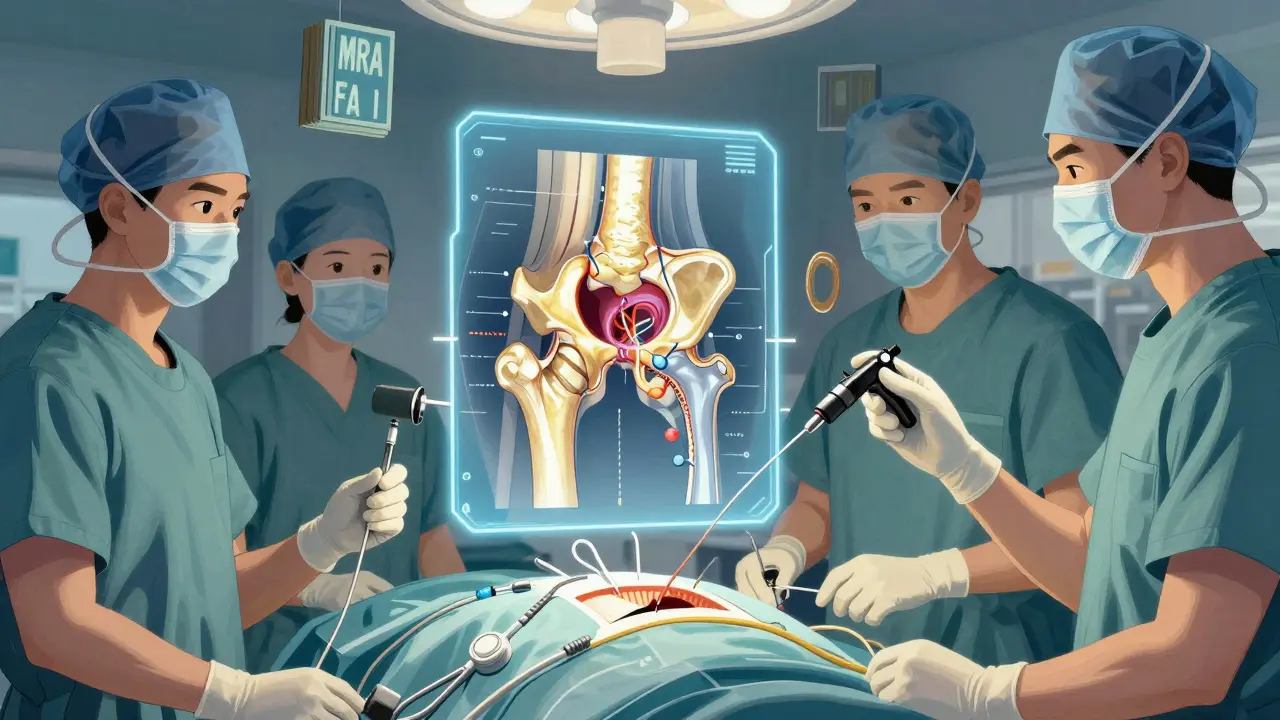
Conservative Treatment: When Surgery Isn’t the First Step
Not every tear needs surgery. If the pain is mild and you’re not pushing hard in sports, doctors often start with conservative care. That means:- Rest - avoiding activities that aggravate the hip for 4-6 weeks
- NSAIDs like ibuprofen or naproxen to reduce inflammation
- Physical therapy focused on hip stability, core strength, and controlled mobility
- Ultrasound-guided corticosteroid injections, which can give 3-6 months of relief in 70-80% of cases
Arthroscopic Surgery: Repair vs. Debridement
There are two main surgical approaches: repair and debridement.- Debridement means trimming away the torn, frayed part of the labrum. It’s quicker and has a shorter recovery - usually 3-4 months back to sport.
- Repair means stitching the labrum back to the bone using tiny suture anchors. This is the preferred option when the tear is clean and the tissue is healthy. Recovery takes longer - 5-6 months - but it preserves the joint’s natural cushioning and reduces long-term arthritis risk.
Special Cases: Hip Dysplasia and Revision Surgery
If you have hip dysplasia - where the socket is too shallow - a labral tear is almost guaranteed. In these cases, repair alone isn’t enough. Surgeons now routinely combine labral repair with a procedure called periacetabular osteotomy (PAO) to reshape the socket. Without this, re-tear rates jump to 60-70%. This isn’t common in all patients, but it’s critical for young athletes with confirmed dysplasia. Missing this step is one of the biggest reasons athletes end up needing revision surgery.
Recovery: What to Expect After Surgery
Recovery isn’t just about waiting. It’s structured. Most programs follow four phases:- Protection (Weeks 1-6): Use crutches, avoid hip flexion beyond 90 degrees, and focus on reducing swelling.
- Strengthening (Weeks 7-12): Start controlled resistance exercises. Quadriceps strength symmetry must reach at least 90% before moving on.
- Sport-Specific Training (Weeks 13-20): Reintroduce cutting, pivoting, and jumping drills under supervision.
- Return to Sport (Weeks 21-26): Only when pain-free, full range of motion is restored, and strength is equal on both sides.
Complications and Long-Term Risks
Hip arthroscopy is generally safe, but it’s not risk-free. About 15-20% of patients still have some pain after surgery. Heterotopic ossification - where bone forms in soft tissue - happens in 5-10% of cases. Nerve injury is rare (1-2%) but possible. And 8-12% of patients need revision surgery within five years, often because the initial diagnosis missed underlying bone issues. The biggest long-term concern? Osteoarthritis. Untreated labral tears increase the risk of hip OA by 4.5 times over 10 years. That’s why fixing the tear - and the cause - isn’t just about getting back on the field. It’s about protecting your hip for life.What’s New in 2026?
The field is evolving fast. In June 2023, the FDA approved a new bioabsorbable suture anchor (Smith & Nephew’s BioX) that dissolves over time, reducing long-term irritation. Early data shows 89% success at two years - better than traditional metal anchors. 3D MRI sequencing is now used in top centers to map complex tears with 97% accuracy. And regenerative therapies like PRP injections are showing promise: one trial found 55% of patients avoided surgery entirely after PRP. The market is booming, too. Over 150,000 hip arthroscopies were done in the U.S. in 2022 - triple the number from 2010. But access isn’t equal. Many athletes pay $1,200-$1,800 out-of-pocket for MRA, while standard MRI costs under $800. That’s a barrier for amateur athletes and those without good insurance.Final Thoughts: Don’t Ignore the Click
A clicking hip isn’t normal. Persistent pain during sports isn’t just ‘bad luck.’ If you’re an athlete and your hip hurts - especially with a catching sensation or deep ache - get it checked properly. Start with X-rays and a physical exam. Push for MRA if symptoms persist. And if surgery is recommended, make sure your surgeon checks for FAI or dysplasia. Don’t settle for a quick fix. Your hip is built to last. Treat it that way.Can a hip labral tear heal on its own without surgery?
No, the labrum doesn’t heal on its own because it has poor blood supply. Mild tears may become less painful with rest and physical therapy, but the tear itself doesn’t repair. Without addressing the root cause - like bone impingement - the injury often worsens over time, increasing the risk of early arthritis.
Is MRI enough to diagnose a hip labral tear?
Standard MRI misses about 30% of labral tears, especially partial-thickness ones. Magnetic resonance arthrography (MRA), which uses contrast dye injected into the joint, is far more accurate - detecting tears with 90-95% sensitivity. For athletes with ongoing hip pain, MRA is the recommended next step after X-rays.
How long does it take to return to sports after hip arthroscopy?
Recovery depends on the procedure. Debridement typically allows return to sport in 3-4 months. Labral repair requires 5-6 months. Full return requires meeting strict milestones: pain-free movement, 90% quadriceps strength symmetry, and full hip internal rotation. Rushing back increases re-injury risk.
What’s the difference between labral repair and debridement?
Debridement trims away the damaged part of the labrum. Repair stitches the torn labrum back to the bone using anchors. Repair is preferred when possible because it preserves the joint’s natural cushioning and reduces long-term arthritis risk. Debridement is faster to recover from but has higher failure rates if underlying bone issues aren’t fixed.
Do I need surgery if I have hip dysplasia and a labral tear?
Yes - and not just a labral repair. Hip dysplasia means the socket is too shallow, which puts constant stress on the labrum. Repairing the labrum without correcting the socket shape leads to a 65% chance of re-tear. Surgeons now combine labral repair with bone reshaping procedures (like PAO) to prevent future failure.
Are PRP injections effective for hip labral tears?
PRP injections show promise for some patients. A 2022 trial found 55% of athletes avoided surgery after PRP and targeted physical therapy. It’s not a cure, but it can reduce pain and inflammation enough to delay or avoid surgery - especially in mild cases or when structural issues are minor.



Donny Airlangga
January 8, 2026 AT 04:43I used to play pickup basketball every weekend until my hip started clicking like a broken hinge. Went to three doctors before someone ordered an MRA. Turned out I had a tear + FAI. Didn't know MRA was the gold standard until I read this. Wish I'd known sooner - could've saved months of pain and bad pivots.
Now I'm 8 months post-repair and back on the court. Rehab was brutal, but worth every second.
Molly Silvernale
January 9, 2026 AT 15:11There’s something profoundly tragic - and beautiful - about the human body: a tiny, avascular ring of cartilage, barely visible on scan, bearing the weight of our dreams… our sprints, our jumps, our pivot-and-shoots… and when it fails, we call it ‘just a tear’ as if it were a sock, not the silent guardian of our joint’s soul.
The labrum doesn’t heal because it’s forgotten by blood, but it doesn’t die - it endures. And so do we. In pain. In PT. In hope. In MRA scans that whisper truth where X-rays lied.
Maybe surgery isn’t about fixing a tear - maybe it’s about honoring the body’s stubborn will to move.
Aubrey Mallory
January 11, 2026 AT 04:15If you’re an athlete and you’re ignoring hip pain because ‘it’ll go away,’ you’re not tough - you’re stupid. I’ve seen too many kids blow out their hips because they didn’t push for MRA. Coaches say ‘play through it.’ Doctors say ‘take NSAIDs.’ But the truth? The labrum doesn’t heal. And if you don’t fix FAI? You’re just buying time until arthritis steals your 30s.
Stop being a hero. Get the scan. Get the consult. Get the repair if you need it. Your future self will thank you - not your Instagram followers.
christy lianto
January 11, 2026 AT 22:44My daughter’s a gymnast - 14, elite level. She started complaining about hip clicking last year. We did everything right: PT, rest, injections. Nothing stuck. Then we found this article. MRA showed a tear + mild dysplasia. Surgeon said ‘repair + watch.’ We did it. She’s 4 months out, back on beam, no pain. The rehab protocol? Exactly as described. 90% quad symmetry? Non-negotiable.
To every parent reading this: don’t let your kid ‘just deal with it.’ This isn’t a sprain. This is a structural crisis. And it’s fixable - if you act fast.
swati Thounaojam
January 12, 2026 AT 07:15in india we dont even get mra easily... my coach said its just muscle pain. i played 6 months with pain. now i need surgery. too late. hope this helps others.
Manish Kumar
January 13, 2026 AT 21:33Let’s be real - this whole thing is capitalism disguised as medicine. We used to just rest and train smarter. Now we’ve got a $1,500 MRA, a $20,000 surgery, bioabsorbable anchors, PRP injections - all marketed to anxious athletes who’ve been told their bodies are fragile. The truth? Most labral tears are asymptomatic. The real problem isn’t the tear - it’s the fear of being broken. We’ve turned athletes into patients before they even need to be.
And yet… I still got mine repaired. Because I was scared too. So maybe I’m the problem.
Dave Old-Wolf
January 14, 2026 AT 05:36Wait - so if you have FAI and you just do debridement, it fails 65% of the time? That’s wild. So the surgeon has to fix the bone AND the labrum? I thought they just trimmed the flappy part. Why isn’t everyone doing the combo? Is it harder? More expensive?
Also, PRP worked for 55%? That’s better than I thought. Maybe worth a try before going under the knife? Just asking.
Prakash Sharma
January 14, 2026 AT 14:41USA spends millions on fancy anchors and MRA while our athletes in India get no access. This is elite healthcare for the rich. My cousin, a state-level hockey player, got told ‘take rest’ for 2 years. Now he can’t even walk without pain. No MRA. No surgery. Just silence. This article is great - but it’s for people who can afford it. What about the rest of us?
Kristina Felixita
January 16, 2026 AT 00:55As a former dancer, I feel this in my bones. The labrum is like the velvet lining of a couture gown - invisible, but essential. When it frays, the whole structure unravels.
And yes - PRP saved me. I did 3 sessions over 3 months. No surgery. Back to barre at 6 months. I’m not saying it works for everyone - but it’s not magic, it’s not hype - it’s biology meeting patience.
Also - if your surgeon won’t check for dysplasia? Find a new one. That’s not optional. That’s non-negotiable.
Joanna Brancewicz
January 16, 2026 AT 14:25FAI + labral tear = biomechanical cascade. MRA is diagnostic gold standard. Debridement without osteoplasty = high re-tear risk. PRP is adjunctive, not curative. Structural correction remains paramount. Rehab protocols must be phase-specific with objective strength benchmarks.
Evan Smith
January 17, 2026 AT 17:53So let me get this straight - you pay $1,800 for an MRA, get surgery, then spend 6 months rehabbing… all so you can go back to jumping and pivoting… just to do it again in 10 years when your hip wears out?
What if we just… stopped playing sports so hard? Just a thought.
Lois Li
January 18, 2026 AT 01:46I’m a physical therapist and I see this all the time. Athletes come in with tears, and the first thing they ask is ‘can I skip rehab?’ No. You can’t. The surgery is only 20% of the battle. The other 80% is doing the boring stuff - clamshells, bridges, hip hikes - every single day. I had a client who returned to soccer at 5 months and re-tore it because he skipped phase 2. Don’t be that person. Your hip isn’t a phone. You can’t just update it.