
Type 2 Diabetes Medication Comparison Tool
Personalize Your Diabetes Treatment
Answer a few questions to find which diabetes medications might be best for you based on your individual needs.
If you're taking Glucophage (Metformin) for type 2 diabetes, you’ve probably noticed it works - but maybe not perfectly. Maybe your blood sugar still spikes after meals, or you’re dealing with stomach upset, or your doctor mentioned it’s not enough anymore. You’re not alone. Millions of people worldwide rely on metformin, but it’s not the only option. So what else is out there? And when should you consider switching?
What Glucophage (Metformin) Actually Does
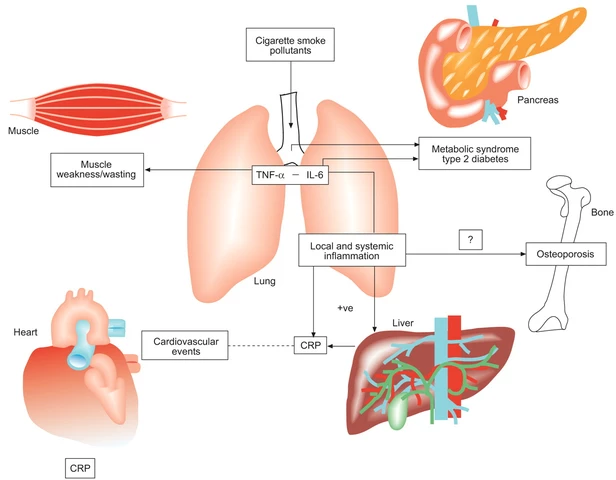
Glucophage is the brand name for metformin, a drug that’s been the first-line treatment for type 2 diabetes since the 1990s. It doesn’t make your body produce more insulin. Instead, it helps your liver stop dumping too much glucose into your blood, makes your muscles better at absorbing sugar, and slows down how fast your gut absorbs carbs. It’s not a quick fix - it works over weeks, not days.
It’s cheap, widely available, and has a strong safety record. Studies show it lowers HbA1c by about 1-2%, reduces heart disease risk, and doesn’t cause weight gain - unlike some other diabetes drugs. But it’s not perfect. Up to 30% of people get digestive side effects: nausea, diarrhea, bloating. Some can’t tolerate even the extended-release version.
When Metformin Isn’t Enough
Many people start on metformin alone. But after a few years, the body adapts. Blood sugar creeps up again. That’s when doctors add another drug. It’s not a failure - it’s normal progression. Type 2 diabetes is a progressive condition. Your pancreas gradually loses insulin-making cells. Your cells become more resistant. Metformin alone can’t always keep up.
Here’s what your doctor might suggest next, depending on your health goals, weight, heart risk, and budget.
SGLT2 Inhibitors: Empagliflozin, Dapagliflozin, Canagliflozin
These drugs - sold as Jardiance, Farxiga, Invokana - work in your kidneys. They make your body pee out extra sugar. That’s it. Simple. And surprisingly powerful.
They lower HbA1c by about 0.5-1%, help you lose 2-5 kg over six months, and reduce heart failure risk by up to 30%. For people with heart disease or kidney problems, they’re often preferred over metformin alone.
Downsides? You might get more yeast infections or urinary tract infections. Rarely, they can cause a dangerous condition called diabetic ketoacidosis, even if your blood sugar isn’t high. You need to stay hydrated. And they cost more - often $100-$150 a month without insurance.
GLP-1 Receptor Agonists: Semaglutide, Liraglutide, Dulaglutide
These are injectables - pens you use once a week or daily. Ozempic, Wegovy, Trulicity. They mimic a gut hormone that tells your brain you’re full and tells your pancreas to release insulin only when needed.
They drop HbA1c by 1-1.8%, help you lose 5-15% of your body weight, and cut heart attack and stroke risk. For someone with obesity and diabetes, they’re game-changers. Some people go from 110 kg to 90 kg in a year.
But they’re expensive. A month of Ozempic can cost $800-$1,200 without insurance. Side effects include nausea, vomiting, and slowed digestion - which can be brutal at first. Not everyone tolerates them. And they’re not approved for everyone - your doctor needs to check your medical history.
DPP-4 Inhibitors: Sitagliptin, Saxagliptin, Linagliptin
These are pills - Januvia, Onglyza, Tradjenta. They boost your body’s own GLP-1 hormone, which helps insulin release after meals.
They’re mild. HbA1c drops by 0.5-0.8%. Weight stays neutral. Side effects are rare. They’re often added to metformin when you need a gentle nudge.
But they don’t help with weight loss. They don’t protect your heart like SGLT2s or GLP-1s. And they’re pricier than metformin. If you’re young, healthy, and just need a small tweak, they’re fine. If you’re at high risk for heart disease? Probably not the best choice.
Thiazolidinediones: Pioglitazone
Pioglitazone (Actos) makes your fat and muscle cells more sensitive to insulin. It’s old, but still used - especially in people with fatty liver disease.
It lowers HbA1c by 0.8-1.2%. But it causes weight gain - 3-8 kg. Increases risk of heart failure. Can weaken bones, raising fracture risk. And it’s been linked to bladder cancer in long-term users.
Most doctors avoid it unless other options have failed. It’s rarely a first add-on anymore.
Sulfonylureas: Glimepiride, Glyburide
These are older drugs - Amaryl, Micronase. They force your pancreas to pump out more insulin.
They work fast. HbA1c drops by 1-2%. And they’re cheap - sometimes under $10 a month.
But here’s the catch: they cause low blood sugar (hypoglycemia). A lot. And they make you gain weight. For older adults, especially those living alone, this is dangerous. Falling, confusion, car crashes - all real risks.
They’re still used, but mostly in places with limited access to newer drugs. Or if someone can’t afford anything else.
Insulin: The Last Resort? Not Always
People think insulin means you’ve “failed” at managing diabetes. That’s not true. Insulin is just another tool. Sometimes it’s the best one.
Long-acting insulins like Lantus or Levemir give steady background control. Fast-acting ones like Humalog cover meals. You can start with just one injection a day.
Insulin lowers HbA1c strongly - often by 1.5-2.5%. But you’ll need to check your blood sugar often. Risk of low blood sugar is real. Weight gain is common.
It’s not scary anymore. Pens are tiny. Injections are quick. Many people feel better once their sugar is steady - fewer brain fogs, more energy.

Which Alternative Is Right for You?
There’s no single best drug. The right choice depends on your goals:
- Want to lose weight? GLP-1s (Ozempic, Wegovy) or SGLT2s (Farxiga, Jardiance)
- Have heart or kidney disease? SGLT2s or GLP-1s - both proven to protect organs
- On a tight budget? Metformin + sulfonylurea (but watch for low blood sugar)
- Prefer pills over shots? DPP-4s or SGLT2s
- Struggling with nausea? Avoid GLP-1s at first - try SGLT2s or DPP-4s
Your doctor might start with one add-on, then adjust. Some people end up on metformin + SGLT2 + GLP-1 - a triple combo that’s powerful and well-studied.
What About Natural Alternatives?
You’ll see ads for cinnamon, berberine, apple cider vinegar. Some studies show small, short-term drops in blood sugar. But none come close to metformin’s proven effect.
Berberine - a plant extract - has been compared to metformin in small trials. It lowers HbA1c by about 0.7-1%, similar to a low-dose sulfonylurea. But it’s not regulated. Quality varies. Can interact with other meds. Not a replacement.
There’s no magic supplement. Lifestyle changes - diet, walking 30 minutes a day, sleep - are the real foundation. Medications just help you stick to it.
What to Do Next
If you’re on Glucophage and it’s not working well, don’t suffer in silence. Talk to your doctor. Ask:
- Is my HbA1c still above 7%?
- Am I having side effects I can’t manage?
- Do I have heart, kidney, or weight issues that could guide a better choice?
- What’s the cost? Is there a generic option?
Bring your blood sugar log. Show your doctor patterns. Maybe your sugar spikes after lunch - that could point to a drug that targets post-meal glucose.
Changing meds isn’t failure. It’s smart management. Your body changes. Your treatment should too.
Final Thoughts
Glucophage (metformin) is still the gold standard - but it’s not the only player. The diabetes toolkit has expanded dramatically. Today, we don’t just lower sugar. We protect your heart, kidneys, and weight. We aim for long-term health, not just numbers on a screen.
If you’re on metformin and it’s working - great. Keep going. If it’s not - you have options. Better ones. Safer ones. Ones that might even help you feel better, not just test better.
Can I stop metformin and switch to a natural remedy?
No. Natural remedies like cinnamon, berberine, or apple cider vinegar may have mild effects, but they don’t replace proven medications. Stopping metformin without medical supervision can lead to dangerously high blood sugar, nerve damage, or kidney stress. Always talk to your doctor before making changes.
Which alternative causes the least weight gain?
SGLT2 inhibitors (like Farxiga and Jardiance) and GLP-1 receptor agonists (like Ozempic and Trulicity) are the best choices. Both help you lose weight - SGLT2s by making you pee out sugar, GLP-1s by reducing appetite. Metformin is neutral. Sulfonylureas and insulin often cause weight gain.
Is it safe to take metformin with another diabetes drug?
Yes. Combining metformin with other drugs is standard practice. Common combos include metformin + SGLT2 inhibitor, metformin + DPP-4 inhibitor, or even metformin + GLP-1. These combinations are studied, effective, and often better than any single drug. Your doctor will check for interactions, especially if you have kidney issues.
Why does metformin cause stomach problems?
Metformin affects the gut directly. It changes how bacteria behave in your intestines and slows digestion. This can cause bloating, gas, and diarrhea - especially when you start. Taking it with food, switching to extended-release, or slowly increasing the dose helps most people. Side effects often fade after a few weeks.
Are there cheaper alternatives to Glucophage?
Yes. Generic metformin is available for under $5 a month in many countries. Other cheap options include sulfonylureas like glimepiride (around $10-$15/month). But cheaper doesn’t always mean better. Newer drugs like SGLT2s and GLP-1s cost more but offer extra benefits - heart protection, weight loss - that can save money long-term by preventing hospital visits.



Tara Stelluti
November 18, 2025 AT 13:43This post is literally a drug company ad disguised as medical advice. They didn't mention the insulin price hike or how pharma bribes doctors with free vacations to push these new GLP-1s. You think you're saving money? You're just getting hooked on a $1000/month luxury.
Margaret Wilson
November 19, 2025 AT 01:49OMG I JUST STARTED OZEMPIC AND I’M LOSING WEIGHT LIKE A ROCKET 🚀 I used to crave donuts every day now I’m just… not hungry? Like what even is food?? My husband says I’m scary now but my A1c dropped from 8.9 to 6.2 so… worth it?? 😭❤️
Mary Follero
November 20, 2025 AT 15:14For real though - if you're on metformin and it's giving you the runs, try the extended-release version. It's a game changer. Also, take it with food. Not right before bed, not on an empty stomach. Just with dinner. And if you're still struggling, talk to your doc about switching to an SGLT2. They're not perfect, but they don't wreck your gut. And yes, they help you lose weight. I dropped 18 lbs in 4 months without trying. Just by taking Farxiga and walking after dinner. Small wins add up.
Abdula'aziz Muhammad Nasir
November 21, 2025 AT 01:34As a healthcare provider in Nigeria, I see patients who rely on metformin because newer drugs are unaffordable. Sulfonylureas are still used out of necessity, not preference. The real issue isn't drug choice - it's access. Many patients stop treatment not because it doesn't work, but because they can't buy it. We need systemic change, not just pharmacological alternatives.
Freddy Lopez
November 21, 2025 AT 20:29Medicine is not a competition between pills. It's a conversation between a human body and a system that's trying to restore balance. Metformin isn't the hero. It's a tool. GLP-1s aren't magic. They're a reflection of our evolving understanding of biology. The real question isn't which drug is best - it's whether we're treating the person, or just the lab value.
Brad Samuels
November 23, 2025 AT 16:37I’ve been on metformin for 8 years. Started with the stomach stuff - terrible. Switched to ER, took it with meals, and now I barely notice it. Then my doc added a low dose of Januvia. My A1c went from 7.8 to 6.4. I still have bad days. But I’m alive. I’m walking my dog every morning. I’m not scared of my next blood test. That’s what matters. Not the brand name. Not the cost. Just showing up.
Will Phillips
November 24, 2025 AT 20:29They don't want you to know this but the FDA approves these drugs because Big Pharma owns them. Metformin is old and cheap so they push the expensive ones. Your doctor gets kickbacks. You think your A1c is down? You're just paying for a marketing campaign. Read the studies - most of them are funded by the drug makers. Wake up. The system is rigged.
Arun Mohan
November 26, 2025 AT 04:39Let’s be honest - if you’re still on metformin after five years, you’re not trying hard enough. I’ve been on semaglutide for 14 months. Lost 32 lbs. My liver enzymes normalized. My energy is insane. Meanwhile, my cousin is still taking glimepiride and complaining about hypoglycemia. You can’t out-supplement your poor lifestyle choices. It’s not about the drug. It’s about discipline. And most people don’t have it.
Tyrone Luton
November 27, 2025 AT 00:16It’s funny how we treat diabetes like a technical problem to be solved with more pills. But what if the real issue is that we live in a world that makes us sick? Processed food. Stress. Sedentary jobs. Sleep deprivation. We’ve created a disease of modernity - and now we’re just patching it with increasingly expensive drugs. The real alternative isn’t another medication. It’s a different way of living. But that’s harder to sell.
Jeff Moeller
November 28, 2025 AT 00:37Metformin works because it’s a blunt instrument. It doesn’t care if you’re sad or tired or stressed. It just slows glucose release. That’s it. The new drugs are fancy. They talk to your brain. They make you lose weight. But they’re not better. Just different. And sometimes different is just more expensive.
Herbert Scheffknecht
November 29, 2025 AT 01:31Here’s the thing nobody says - most people don’t need a new drug. They need a new routine. Walk after dinner. Sleep 7 hours. Stop drinking soda. Eat veggies. It’s boring. It’s not sexy. But it works better than any pill. I’ve seen it. I’ve done it. I’ve helped others do it. You don’t need Ozempic. You need consistency. And that’s the hardest part.
Jessica Engelhardt
November 30, 2025 AT 03:16Who even needs metformin anymore? I’m on a keto diet and berberine and I haven’t taken a pill in 2 years. My A1c is 5.1. My doctor says I’m a miracle. But I know the truth - Big Pharma doesn’t want you to know that food is medicine. They want you dependent. I’m free. You can be too. Just cut the carbs. Stop trusting the system. You’re smarter than they think.
william volcoff
December 1, 2025 AT 12:07Just to clarify - if you’re on metformin and it’s working, don’t fix what ain’t broke. But if you’re having side effects or your A1c’s creeping up, it’s not weakness to ask for something else. The medical system loves to make you feel guilty for needing help. You’re not failing. You’re adapting. And that’s smart.
Freddy Lopez
December 2, 2025 AT 17:36There’s a quiet dignity in managing a chronic condition with patience. Not every solution needs to be dramatic. Sometimes the most radical act is simply showing up - taking your pill, walking your dog, checking your numbers - without fanfare. The drugs are tools. The discipline is the art.