What Happens to Your Lungs After COVID-19?
Most people recover from COVID-19 without lasting issues. But for many, breathing problems don’t go away. Even if you didn’t need hospital care, you might still feel short of breath, tired after walking a few steps, or like you can’t catch your full breath. This isn’t just fatigue-it’s your lungs still healing, or in some cases, damaged.
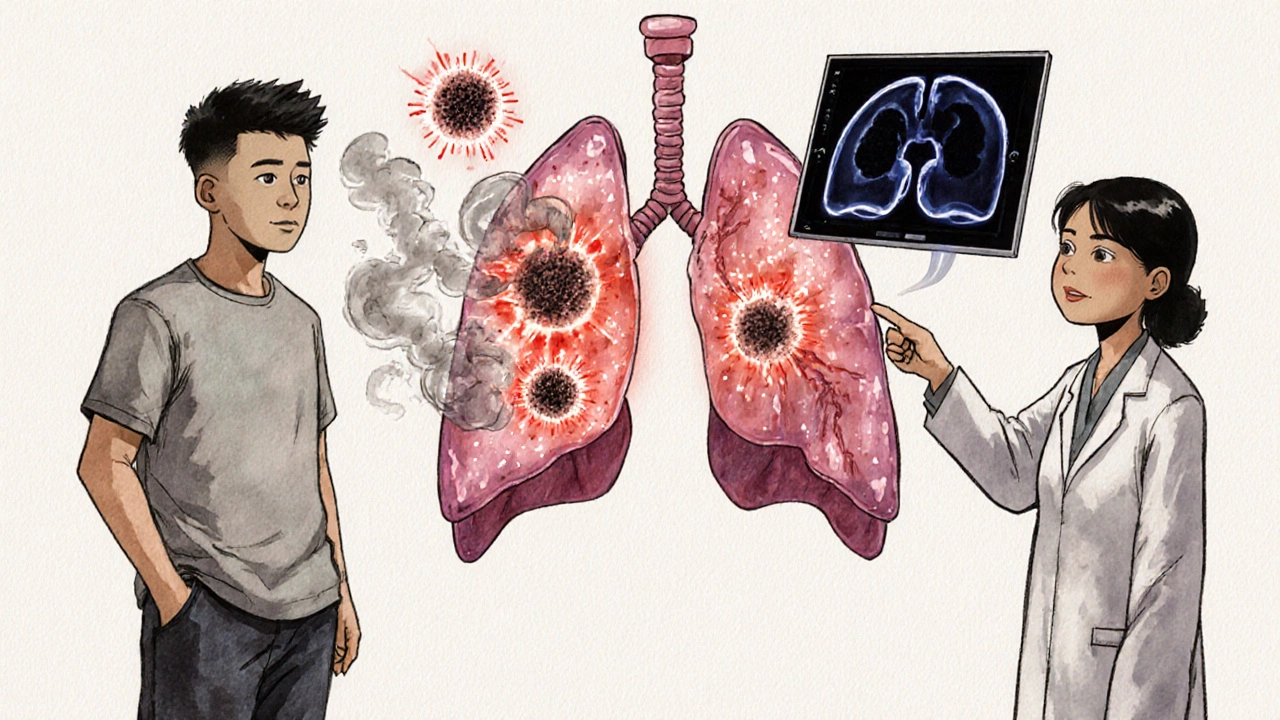
Research from the Centre for Heart Lung Innovation (HLI) in 2025 shows that about one-third of long COVID cases involve the lungs. These aren’t just vague symptoms. There’s real, measurable damage happening in the smallest airways-the places regular X-rays and lung function tests can’t see. The virus may be gone, but your immune system is still reacting. Specifically, a type of white blood cell called a neutrophil keeps firing off inflammation signals like a dirty bomb, even after the virus is cleared. This keeps damaging the tiny air sacs where oxygen enters your blood.
Who’s Most at Risk for Lasting Lung Damage?
Not everyone gets the same effects. People who were hospitalized, especially those who needed oxygen or a ventilator, face higher risks. A South Korean study of over 5,700 hospitalized adults found that 12.6% developed post-COVID pulmonary fibrosis (PCPF)-permanent scarring in the lungs. That’s about 1 in 8. And even among those who didn’t need intensive care, 30.4% still had breathing problems three months after leaving the hospital, according to an Italian study.
But it’s not just about severity of the initial infection. People with pre-existing lung conditions like COPD are at much higher risk. One 2025 study showed they had a 4.6% death rate after COVID-19, compared to 0% in COPD patients who didn’t get infected. They also had more flare-ups and higher rates of heart failure afterward.
Interestingly, needing a ventilator didn’t make lung damage worse than just needing oxygen. That means even moderate cases can lead to long-term issues. The real predictor? How bad your breathing felt early on. If your breathlessness score (mMRC ≥2) was high one month after infection, you were far more likely to keep struggling months later.
Why Standard Tests Miss the Problem
If your chest X-ray looks normal and your spirometry test shows "normal" lung function, doctors might tell you there’s nothing wrong. But that doesn’t mean you’re fine. Traditional tests can’t see what’s happening in the tiniest airways-the alveoli-where oxygen actually moves into your bloodstream.
This is where hyperpolarized xenon MRI changes everything. This advanced imaging lets doctors watch oxygen move through the lungs in real time. Studies from HLI and Duke University show that people with long COVID have clear gaps in oxygen transfer, even when other tests look okay. It’s like your lungs have invisible leaks. That’s why you feel out of breath climbing stairs, even if your lung capacity numbers look fine on paper.
There are four distinct patterns of this oxygen transfer failure, identified through xenon MRI. That means not everyone’s long COVID lung damage looks the same. One person might have trouble with air sacs, another with the tiny tubes leading to them. This is why a one-size-fits-all treatment doesn’t work.
What Does Rehabilitation Actually Look Like?
Recovery isn’t just rest. It’s structured, guided rehab. Most programs start at least four weeks after the acute phase and last 8 to 12 weeks, with sessions two or three times a week. These aren’t gym workouts-they’re carefully designed programs that rebuild your lung function and stamina without pushing you too far.
A typical program includes:
- Breathing retraining-learning how to use your diaphragm properly instead of shallow chest breathing
- Aerobic conditioning-low-intensity walking, cycling, or swimming to slowly rebuild endurance
- Strength training-focusing on arms and legs to reduce the effort needed for daily tasks
- Education-understanding pacing, energy conservation, and how to recognize when you’re overdoing it
Studies from the Lung Foundation Australia show that people who complete these programs see real improvements: better FEV1 (how much air you can blow out), improved diffusion capacity (how well oxygen enters your blood), and longer 6-minute walk distances. They also report less breathlessness and more energy.
For people with COPD or heart issues, programs are adjusted. Monitoring is tighter. Progress is slower. But it still works.
How Do You Know If You’re Getting Better?
Progress isn’t always measured in numbers. You’ll know you’re improving when:
- You can walk to the mailbox without stopping
- You can shower without needing to sit down afterward
- You can talk in full sentences without gasping
- You sleep through the night without waking up breathless
Doctors use tools like the 30-second sit-to-stand test (30STS) to track functional changes. People with severe long COVID can do fewer repetitions. As you recover, that number climbs. It’s a simple, reliable way to measure real-world improvement.
Also, keep track of your mMRC score-this is a 4-point scale that asks how often you get breathless during daily activities. If your score drops from 3 to 1 over three months, that’s meaningful progress.

What About Medications? Can They Help?
There’s no magic pill yet. But research is pointing to promising directions. In the South Korean study, patients who got remdesivir during their acute infection were less likely to develop lung scarring. Those who got baricitinib had a higher risk-but researchers think this might be because it was given to sicker patients, not because the drug itself caused harm.
What’s exciting is what’s coming next. The RECOVER Initiative is launching clinical trials in 2025-2026 to test drugs that target neutrophils-the immune cells causing ongoing damage. If they work, these could stop the inflammation before it turns into permanent scarring.
For now, avoid unproven supplements or high-dose steroids. They haven’t been shown to help and can cause side effects. Stick with rehab, pacing, and medical supervision.
What’s the Long-Term Outlook?
The good news? Most people get better over time. Lung function improves noticeably by six months for those with moderate to severe infections. Many return to near-normal activity levels.
The bad news? About 12.6% of hospitalized patients develop permanent fibrosis. That means lifelong management-regular check-ups, possible oxygen therapy, and avoiding lung irritants like smoke or pollution.
And it’s not just the lungs. Long COVID with breathing problems is linked to higher risks of kidney disease, heart strain, and mental health challenges. That’s why rehab programs now include mental health support and nutrition advice, not just breathing exercises.
Research is moving fast. The American Thoracic Society and European Respiratory Society are finalizing official guidelines for diagnosing and treating pulmonary long COVID, expected by late 2025. Hospitals are starting to set up dedicated long COVID clinics with access to xenon MRI and specialized rehab teams.
What Should You Do Now?
If you’re still having breathing issues after a COVID-19 infection:
- Don’t ignore it. Persistent breathlessness isn’t normal.
- See a pulmonologist. Ask about pulmonary rehab and whether advanced imaging (like xenon MRI) is available.
- Start slow. Walk for 5 minutes a day. Add 1 minute each week. Don’t push through breathlessness.
- Track your symptoms. Use a journal or app to note when you feel out of breath, what you were doing, and how long it took to recover.
- Join a rehab program. Even if your doctor says "it’s just fatigue," ask for a referral. Programs exist for a reason-and they work.
You’re not alone. Thousands are walking this path right now. Recovery isn’t linear. Some days are better than others. But with the right support, most people find their way back to a full, active life.



Conor McNamara
November 19, 2025 AT 01:04my cousin got covid and now she cant climb stairs. she says its her lungs but i think its the chips. theyre watching us.
steffi walsh
November 19, 2025 AT 23:18ps: if you're reading this and feeling hopeless, i believe in you. you're not alone 🌈
Leilani O'Neill
November 20, 2025 AT 03:29And don't get me started on this 'xenon MRI' nonsense. That's expensive nonsense for people who can't accept that their lungs are just tired. Get a grip.
Riohlo (Or Rio) Marie
November 21, 2025 AT 23:33Meanwhile, real science is quietly documenting that neutrophil dysregulation is the key, not some 12-week rehab program that sounds like a spa brochure. And don't even get me started on the fact that they're calling it 'long COVID' like it's a lifestyle brand. It's a systemic immune collapse, sweetheart. Not a wellness trend.
Brenda Kuter
November 22, 2025 AT 11:39People who dismiss this as "just fatigue" are either uninformed or willfully ignorant. The data is here. The tools exist. The path forward is clear. Stop blaming the victim. Start supporting the science.
Iska Ede
November 24, 2025 AT 02:12also why is it that every time someone says "research shows" it turns out to be a 3-page PDF from a university newsletter? i'm not buying the hype. i'm still breathing. barely. but i'm breathing.
Gabriella Jayne Bosticco
November 24, 2025 AT 14:29Don’t wait for a perfect test. Start small. Walk to the mailbox. Sit down if you need to. Breathe slow. You’re not broken. You’re rebuilding. And that’s okay.
Katelyn Sykes
November 26, 2025 AT 10:47also the breathing retraining thing? game changer. i didnt even know i was breathing wrong. now i feel like i have 2 lungs instead of 1.
if you're reading this and feel hopeless - start with 2 minutes a day. you can do it
Gabe Solack
November 28, 2025 AT 07:01my wife had covid in 2021 and we thought she'd bounce back. she didn't. she's been doing rehab for a year now. the xenon MRI showed gaps in her lungs we never knew existed.
don't let anyone tell you it's "all in your head." your lungs are healing. it's slow. it's messy. but it's real. 🙏
Shaun Barratt
November 30, 2025 AT 03:28That said, the claim that 30.4% of non-hospitalized patients experienced persistent dyspnea at three months is consistent with longitudinal data from the UK's COVID-19 Long Term Effects Cohort.
Recommendation: If your primary care provider dismisses your symptoms, request a referral to a pulmonary rehabilitation center. Do not self-diagnose. Do not rely on anecdotal evidence. Evidence-based care exists.