Understanding Albuterol and Asthma
Asthma is a chronic respiratory condition that affects millions of people worldwide. It can be challenging to manage and may require the use of various medications to control symptoms and prevent asthma attacks. Albuterol is one of the most commonly prescribed medications for asthma, but there are also other options available. In this article, we will discuss the differences between albuterol and other asthma medications, so you can make an informed decision about your asthma treatment plan.
What is Albuterol?
Albuterol is a type of bronchodilator medication that is used to treat asthma and other respiratory conditions. It works by relaxing the muscles in the airways, allowing for easier breathing. Albuterol is available in various forms, including inhalers, nebulizers, and tablets. It is often prescribed as a rescue medication to be used during an asthma attack or when symptoms suddenly worsen.
Types of Asthma Medications
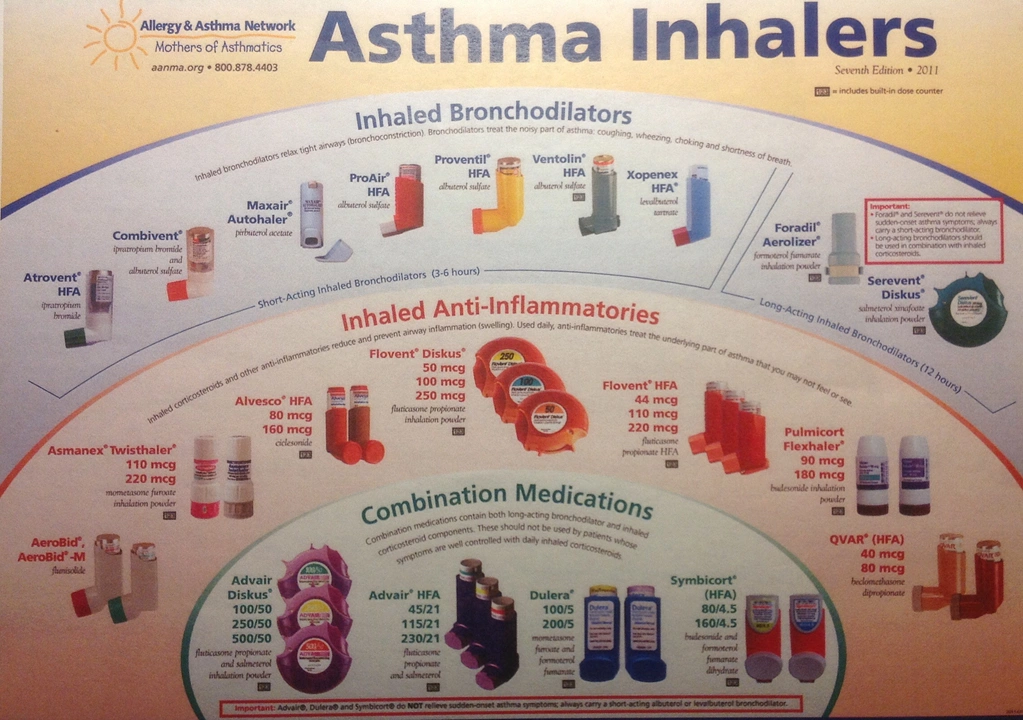
There are several types of asthma medications available, and they can be divided into two main categories: quick-relief medications and long-term control medications. Quick-relief medications, like albuterol, are used to treat sudden symptoms and are typically taken on an as-needed basis. Long-term control medications are taken daily to manage asthma symptoms and prevent asthma attacks. These medications include inhaled corticosteroids, long-acting beta-agonists, and leukotriene modifiers.
Inhaled Corticosteroids: A Long-Term Control Option
Inhaled corticosteroids are a type of long-term control medication that is used to reduce inflammation in the airways. They are considered the most effective long-term control medication for asthma and are typically the first-line treatment for people with persistent asthma. Examples of inhaled corticosteroids include fluticasone, budesonide, and beclomethasone. These medications are usually taken daily, and it may take several weeks for their full effects to be felt.
Long-Acting Beta-Agonists: Another Long-Term Control Option
Long-acting beta-agonists (LABAs) are another type of long-term control medication that is used to treat asthma. They work similarly to albuterol by relaxing the muscles in the airways, but they have a longer duration of action. LABAs are often prescribed in combination with inhaled corticosteroids for people with moderate to severe asthma. Examples of LABAs include salmeterol and formoterol.
Leukotriene Modifiers: An Alternative Long-Term Control Option
Leukotriene modifiers are another type of long-term control medication that can be used to treat asthma. They work by blocking the action of leukotrienes, which are chemicals that cause inflammation and constriction of the airways. Leukotriene modifiers are taken in pill form and may be a good option for people who have difficulty using inhalers. Examples of leukotriene modifiers include montelukast, zafirlukast, and zileuton.
Combination Medications for Asthma Control
For some people with asthma, a combination of medications may be necessary to achieve optimal control of their symptoms. Combination medications typically include an inhaled corticosteroid and a long-acting beta-agonist, which work together to reduce inflammation and relax the airways. Examples of combination medications include fluticasone/salmeterol, budesonide/formoterol, and mometasone/formoterol.
Choosing the Right Asthma Medication for You
There is no one-size-fits-all approach to treating asthma, and the medications that work best for one person may not be as effective for another. When choosing an asthma medication, it is essential to consider factors such as your asthma severity, your preferences for administration (inhaler, nebulizer, or pill), and any potential side effects. It's important to work closely with your healthcare provider to develop a personalized asthma action plan that includes the most appropriate medications for your specific needs.
Managing Asthma with Lifestyle Changes and Avoiding Triggers
In addition to medication, managing your asthma effectively may also involve making certain lifestyle changes and avoiding triggers that can cause your symptoms to worsen. This may include quitting smoking, maintaining a healthy weight, identifying and avoiding allergens like pollen and pet dander, and reducing exposure to air pollution. By working with your healthcare provider and making these adjustments, you can help to control your asthma and improve your overall quality of life.

Jonathan Debo
April 29, 2023 AT 16:18Albuterol is, unequivocally, the gold standard-though I’m astonished that the article didn’t cite the 2022 GINA guidelines, which explicitly recommend against monotherapy with SABAs in persistent asthma. The over-reliance on albuterol is a public health crisis, and it’s frankly irresponsible not to emphasize that it’s a band-aid, not a cure.
Patients who use albuterol more than twice a week without a controller medication are statistically at higher risk of near-fatal exacerbations. This isn’t opinion-it’s meta-analysis data from The Lancet Respiratory Medicine. If you’re not on an ICS, you’re playing Russian roulette with your lungs.
And yes, I’ve seen it: the guy who buys three albuterol inhalers a month, then wonders why he’s in the ER every spring. No, it’s not the pollen-it’s the lack of maintenance therapy.
Also, the article mentions LABAs-but omits the FDA black box warning. You don’t prescribe formoterol without an ICS. Period. End of sentence. No exceptions.
Montelukast? Fine for mild cases, but it’s not for someone with FEV1 under 60%. And don’t even get me started on the neuropsychiatric side effects. I’ve had two patients develop severe depression on it. One quit meds entirely. Don’t be that doctor.
Combination inhalers? Yes, absolutely. But only if the patient can coordinate inhalation. Most can’t. Which is why nebulizers still have a place-especially in the elderly. Don’t let tech bros tell you inhalers are always superior.
And yes, lifestyle changes matter-but not because “you should eat more kale.” It’s because obesity increases airway inflammation independently. Weight loss of 5–10% improves asthma control more than adding a third medication.
Also: stop calling albuterol a “rescue” drug. It’s a symptom suppressor. The real rescue is the fluticasone you’re not taking.
Finally-please, for the love of all that is pulmonary-stop using the term “mild asthma.” There’s no such thing. There’s only well-controlled and poorly controlled. And if you’re using albuterol weekly, you’re not in the former.
And if you’re still using oral steroids for routine flares? You need a new pulmonologist.
Melissa Delong
April 29, 2023 AT 19:57I don't trust albuterol. I read online that it's been linked to heart problems in children. And the FDA? They're controlled by big pharma. They approved it because they get money from the makers. I know someone who had a seizure after using it. They never told you that in the article.
Also, I think asthma is caused by 5G towers and vaccines. The real cure is magnesium and lemon water. No one wants to tell you that.
Marshall Washick
April 30, 2023 AT 08:36I’ve been on albuterol since I was six. I remember the first time I used a nebulizer-my mom crying because she thought I wouldn’t breathe. I’m 34 now. I’ve been on fluticasone for 12 years. I don’t use albuterol more than twice a month. It’s not about being scared of meds. It’s about being smart with them.
I don’t know why this article didn’t mention how expensive these inhalers are. My co-pay is $85. I know people who skip doses because they can’t afford it. That’s the real crisis.
I wish more doctors would say: ‘You’re not weak for needing a controller. You’re smart.’
Abha Nakra
May 1, 2023 AT 16:17As someone who grew up in India with no access to inhalers until I was 18, I can say this: albuterol saved my life. But I also know people who used it daily for years because they had no access to steroids. It’s not just about the science-it’s about equity.
Here in the U.S., we talk about LABAs and ICS like they’re universal. But in rural India, a child with asthma might get a tablet of theophylline and a prayer. I’m grateful for what we have here-but I wish we’d talk more about global access.
Also, montelukast is a game-changer for kids who hate inhalers. My niece takes it. She’s been asthma-free for three years. No nebulizer. No stress. Just a pill before bed.
And yes, avoiding smoke and dust matters. But so does having a job that doesn’t make you choose between rent and your inhaler.
Neal Burton
May 3, 2023 AT 04:05Albuterol is overprescribed because doctors are lazy. They don’t want to spend 20 minutes explaining controller meds. So they hand out a blue inhaler like it’s candy. Meanwhile, patients are dying because they think ‘rescue’ means ‘permanent solution.’
The real problem? The pharmaceutical industry profits more from rescue inhalers than from controllers. Why? Because you need to buy a new one every 3 months. A steroid inhaler lasts a year.
And don’t get me started on the marketing. ‘Quick relief!’ ‘Fast acting!’ ‘Feel better now!’ It’s all designed to keep you dependent.
I’ve seen patients who’ve used 47 inhalers in five years. All of them were prescribed by different doctors. No one connected the dots.
This isn’t medicine. It’s a business model.
Tamara Kayali Browne
May 3, 2023 AT 21:28There is a statistically significant correlation between increased albuterol use and emergency department visits (p < 0.001). The article fails to acknowledge that albuterol monotherapy is associated with a 2.3x higher risk of asthma-related hospitalization compared to ICS/LABA combination therapy. Furthermore, the absence of data on adherence rates undermines the entire premise. Without adherence metrics, any recommendation is speculative.
Additionally, the mention of leukotriene modifiers ignores the fact that montelukast has a 12% discontinuation rate due to neuropsychiatric adverse events, per the FDA’s 2020 safety review. This is not a benign option. The article’s tone is dangerously optimistic.
Nishigandha Kanurkar
May 4, 2023 AT 04:07Albuterol is a government weapon! They put it in the air to make people dependent so they’ll buy more drugs! The inhalers have microchips that track your breathing-and then send data to the WHO! That’s why they say it’s safe-because they control the data!
And the ‘steroids’? They’re not steroids-they’re nanobots that turn your lungs into robots! That’s why you need to take them every day! They’re reprogramming you!
I’ve seen the videos. The doctors are paid by the Illuminati. The ‘asthma’ is just a distraction so you won’t notice the 5G towers are melting your brain!
Stop taking it! Drink apple cider vinegar and sleep in a Faraday cage!
Lori Johnson
May 5, 2023 AT 09:56Just wanted to say-this article made me feel seen. I used to be terrified of steroids. I thought they’d make me gain weight or turn me into a monster. But after my doctor explained it to me like I was a person-not a chart-I started fluticasone. I haven’t been to the ER in 3 years.
It’s not magic. It’s just… better. And I wish more people knew that.
Also, if you’re struggling with cost? Ask for samples. Ask for coupons. Ask your pharmacist. There are programs. You’re not alone.
Tatiana Mathis
May 6, 2023 AT 05:45Thank you for writing this. I’ve been managing asthma since childhood, and I’ve seen the evolution-from nebulizers that looked like sci-fi machines, to today’s sleek inhalers with dose counters. But what hasn’t changed is how little most people understand about the difference between rescue and control.
I’ve had coworkers ask me why I don’t just ‘get over it.’ I’ve had teachers tell me I was faking it to avoid gym. I’ve had ER nurses roll their eyes when I asked for a nebulizer because my inhaler ‘wasn’t working.’
Albuterol isn’t the enemy. But treating it like the solution? That’s the problem. I’m not proud of the years I spent using it daily because I didn’t know better. I’m proud of the years I’ve spent using my controller and living fully-hiking, traveling, teaching, dancing.
If you’re reading this and you’re on albuterol more than twice a week? Please, talk to your doctor. Not tomorrow. Today. You deserve to breathe without fear.
And if you’re a provider? Don’t just hand out prescriptions. Ask: ‘What’s your life like when you’re not having an attack?’ That’s the question that changes everything.
Also-yes, avoiding triggers matters. But so does having a job that doesn’t make you choose between rent and your inhaler. And yes, I know someone who got their inhaler for $5 through a patient assistance program. You can too.
Let’s stop treating asthma like a personal failure. It’s a medical condition. And we have the tools to manage it. We just need to use them-wisely, compassionately, and together.